A record of a Patient's health, past illnesses, medical conditions, and treatments they have received or undergone. The History typically includes information about the Patient's personal medical background, family medical history, and any current symptoms or complaints. The History can be collected and maintained by the Practice. Having a Patient's History is important for Practitioners and other healthcare providers in diagnosing and treating medical conditions, and can be beneficial to help identify potential risk factors for certain diseases or conditions.
Please Note: The information in this user manual relates directly to the Eye Evaluation 2 form.
The contents of this user manual will consist of the following information:
Family History
Opthalmic History
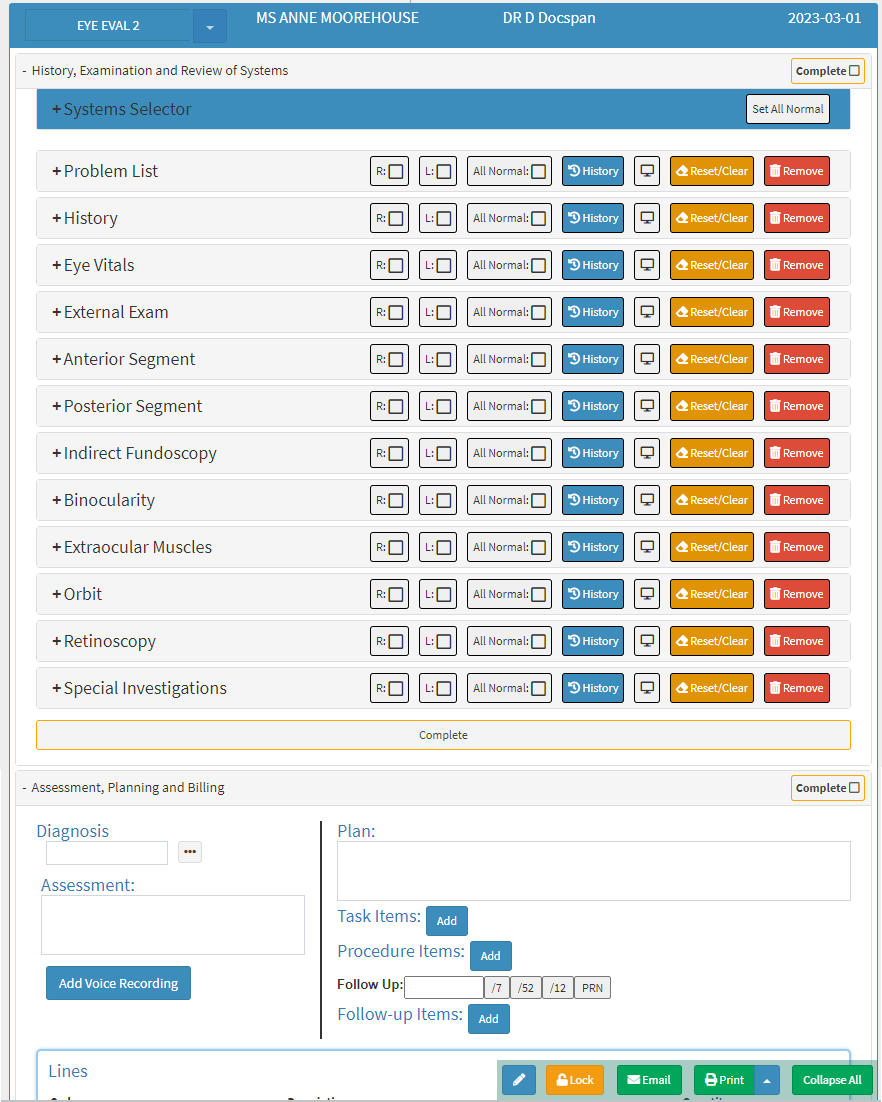
This user manual will start on the Eye Evaluation 2 Form.
For more information regarding how to Navigate to the Eye Evaluation 2 form, please refer to the user manual: Eye Evaluation 2 Form Overview.
Click on the History panel.
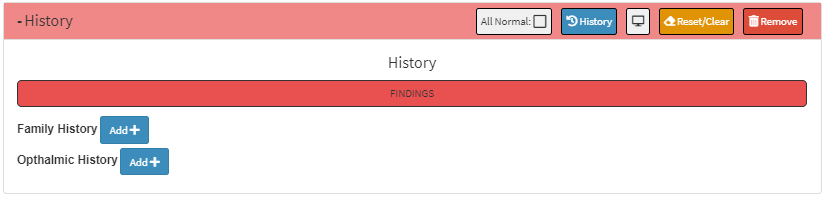
The History panel will expand.
Please Note: When no information has been added to the History panel, the state of the panel will always be Unchecked.
Click on the Unchecked button to open all the features of the History panel to be able to enter the desired findings.
The History panel will be highlighted in red to show that findings have been added to the History panel.
An explanation will be given for each field and option on the History panel:
Findings: Gives an indication that abnormal conclusions have been made.
Click on the Findings button to indicate Normal findings in the History panel.
The Findings button will change to green to show that the conclusion which has been made is Normal.
Please Note: When the user clicks on the Normal button all the extra options on the History panel will close and the panel will be marked as Unchecked.
Family History
A record of hereditary illnesses and conditions that run in the Patient's family, such as Heart Disease, Retinitis Pigmentosa etc. For more information regarding a Patient's Family History, please refer to the user manual: General History.
Click on the Add + button to add the information regarding the Patient's Family History.
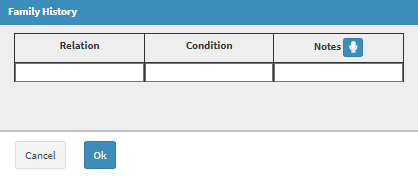
The Family History screen will open.
An explanation will be given for each field and option on the Family History screen:
Relation: The connection between the Patient and their family member, for example, Mother, Father, Brother and sister etc.
Click on the Relation field to enter the relevant information.
Condition: The medical condition that relates to the family member that was completed in the Relation field.
Click on the Condition field to enter the name of the condition.
Notes: Any extra information that relates to the particular condition of the Patient's family member.
Click on the Notes field to enter any relevant information.
Click on the Microphone button to transcribe an audio note to the Notes field.
For more information regarding how to transcribe voice notes, please refer to the user manual: Add Voice Recording.
Click on the Cancel button to close the Family History screen without saving and return to the Eye Eval 2 screen.
Click on the Ok button to save the changes which have been made.
The fields which were completed will now appear in the Family History section. The Family History sectionis a persistent section which remembers the information which has been added to the field even if the screen has been saved and closed, allowing the Practitioner to see the information every time the form is opened.
Click on the Delete button to remove the entry from the list.
Please Note: The Practitioner is able to add as many lines as desired to the Family History section as desired/necessary, following the steps as explained above.
Opthalmic History
A detailed record of a Patient's eye and vision-related symptoms and past history thereof.
Click on the Add + button to add the information regarding the Patient's Ophthalmic History.
TheOphthalmic History screen will open.
An explanation will be given for each field and option on the Ophthalmic History screen:
Condition: The name of the medical condition which is affecting the Patient's eye and/or vision.
Clickon theCondition field to enter the name of the condition.
Eye: The eye which is affected by the condition.
Click on the relevant option which is available in the Eye field.
Right: The eye on the right side of the face is affected.
Left: The eye on the left side of the face is affected.
Both: The eye on the left and right side of the face are both affected.
Duration: How long the Condition has been affecting the Patient
Click on the Duration field to enter the number of days/weeks/months/years which the Patient has been experiencing the condition/symptoms.
Onset: When the Patient started to notice the symptoms which they are experiencing.
Click on the Onset field to enter when the Patient started experiencing symptoms of the condition.
Severity: How bad the condition is, which is affecting the Patient.
Click on theSeverity field to enter how badly the condition/symptoms has affected the Patient.
Impact: The consequences of the condition for the Patient.
Click on the Impact field to enter how the Patients' life has been affected.
Phases: To what degree the condition has progressed.
Click on the Phases field to enter the relevant information regarding what degree the patient has been affected.
Note: Any extra information that relates to the particular condition of the Patients.
Click on the Notes field to enter any relevant information.
Click on the Microphone button to transcribe an audio note to the Notes field.
For more information regarding how to transcribe voice notes, please refer to the user manual: Add Voice Recording.
Click on the Cancel button to close the Ophthalmic History screen without saving and return to the Eye Eval 2 screen.
Click on the Ok button to save the changes which have been made.
The fields that have been completed will now appear in the Ophthalmic History section. The Ophthalmic History sectionis a persistent section which remembers the information which has been added to the field even if the screen has been saved and closed, allowing the Practitioner to see the information every time the form is opened.
Click on the Delete button to remove the entry from the list.
Please Note: The Practitioner is able to add as many lines as desired to the Ophthalmic section as desired/necessary, following the steps as explained above.