The purpose of the EMR Form is to provide decision support to healthcare professionals with respect to the rendering of healthcare services to an individual patient and accommodate data exchange in the Emergency Room.
- Log in to the GoodX WebApp using your GoodX username and password.
- From the Diary >> click on the patient booking >> the Sidebar will appear on the right-hand side of the screen.
- Click on the Clinical button
- From the Forms library select the EMR form to complete.
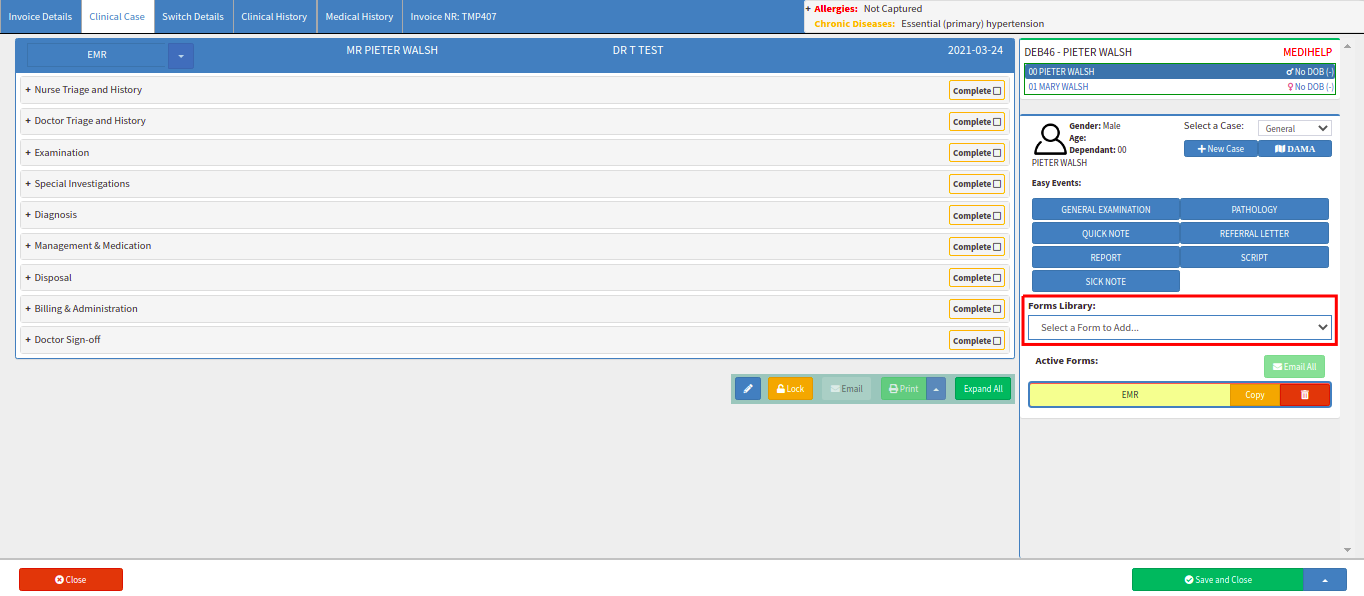
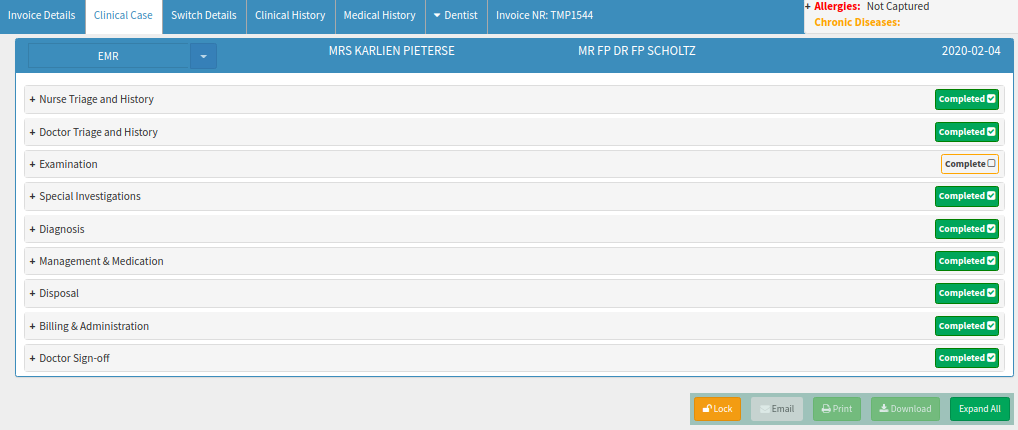
EMR Form Sections Explained:
- Nurse Triage and History: refers to the formal process of early assessment of the patients attending an accident and emergency department by a trained and qualified nurse, to ensure that they receive appropriate attention, in a suitable location, with the requisite degree of urgency. The patient's Vitals will be completed in this section.
- Doctor Triage and History: refers to the formal process of early assessment of the patients attending an accident and emergency department by a trained and qualified Doctor, to ensure that they receive appropriate attention, in a suitable location, with the requisite degree of urgency. The patient's Vitals will be completed in this section by the Doctor or the Doctor can accept the Vitals that were done by the Nurse.
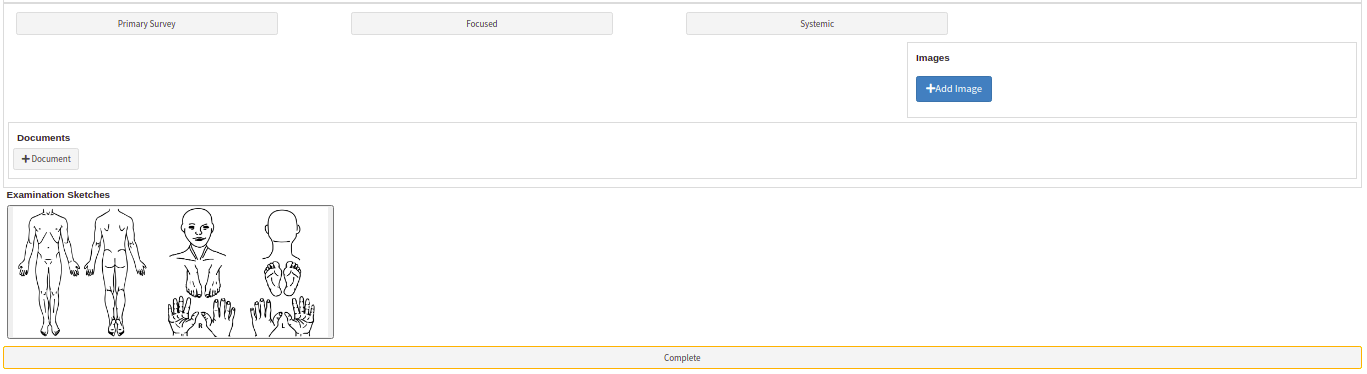
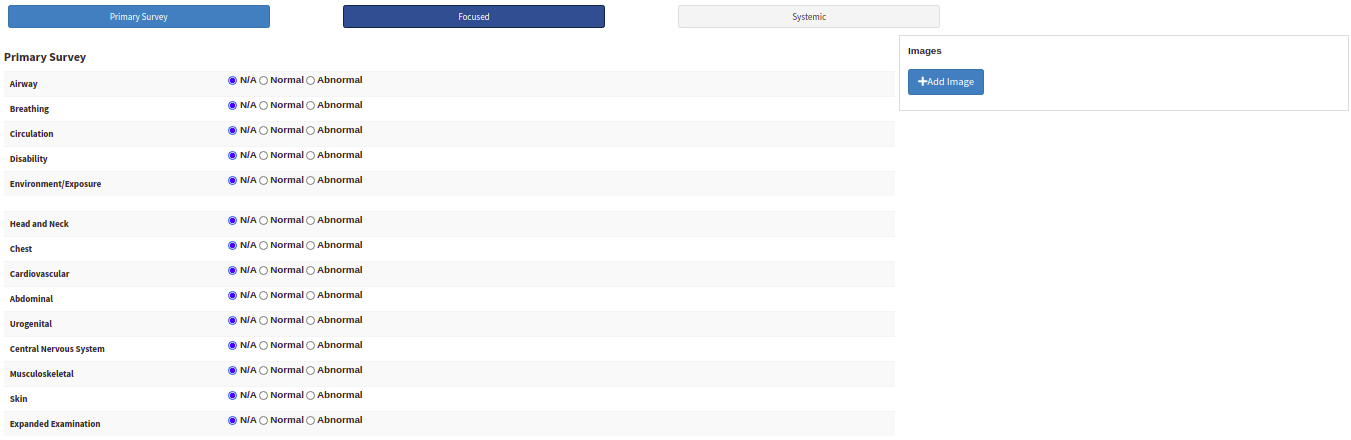
- Examination: In the physical/medical examination, the doctor examines the patient for any possible medical signs or symptoms of a medical condition or accident. In this section, the Doctor can add images related to the illness or injury or mark the sketches provided after examining the Patient.
- Special Investigation: After the patient's vitals and physical examination were done the Doctor might send the patient for more tests to determine a diagnosis. In this section the Doctor can send the patient for blood works, x-rays or any other scans or tests required.
- Diagnosis: In this section, the Doctor will know and complete the diagnosis by identifying the nature of the patient's illness or other problems. He will complete the case type and case subtype and complete the ICD-10 code related to the diagnosis.
- Management and Medication: the purpose of this section is to help the Doctors and regulators to focus on mitigating the risks for medication management in the emergency room. Reducing opportunities for medication error and increasing the opportunities for a safe medication management environment represents a prime opportunity to improve the healthcare delivery system. You will complete and issue a script from here for the Patient.
- Disposal: In this section, you will complete what happened to the Patient while they were in the ER. Were they admitted to the Hospital, Discharged, Transferred to another facility, Died, etc. Under every option is a section that needs to be completed.
- Billing and Administration: In this section, the billing for the consultation and procedures will be done after the Doctor has discharged the patient from the ER. It will either be submitted to Medical Aid or the Patient will settle the account then and there before leaving the emergency room.
- Doctor Sign-Off: The Doctor will add his signature to the EMR Form after every section was completed to sign off the form.
- Nurse Triage and History: refers to the formal process of early assessment of the patients attending an accident and emergency department by a trained and qualified nurse, to ensure that they receive appropriate attention, in a suitable location, with the requisite degree of urgency. The patient's Vitals will be completed in this section.

Take Note: Under the Override TEWS icons, when either Ward, High Care or ICU is set as the Override TEWS, a trigger will set
the booking type on the Diary to ‘Ward Visit’.
The Override TEWS will always override the booking type on the Diary if it is set up correctly. Make sure that 'Ward Visit' Booking Type with the color is setup under Settings >> Diary Settings >> Booking Type Setup >> Add new type >> Ward Visit >> Change colour to purple (#899AFF). If this booking type is not set up the trigger will not override the booking type in the Diary when Ward / High Care / ICU is selected on the EMR form.
This trigger on the diary will only occur when this is set in the Doctor Triage and History section. Only when the user marks the Doctor Triage and History as Completed will the trigger update the booking type to ‘Ward Visit’ on the Diary.

- Doctor Triage and History: refers to the formal process of early assessment of the patients attending an accident and emergency department by a trained and qualified Doctor, to ensure that they receive appropriate attention, in a suitable location, with the requisite degree of urgency. The patient's Vitals will be completed in this section by the Doctor or the Doctor can accept the Vitals that were done by the Nurse.

Take Note: As with all values, the selection of the Override TEWS in the Nurse Triage and History will be copied to the Doctor Triage and History when the button ‘ACCEPT NURSE VITALS’ is clicked in the Doctor Triage and History > DOCTOR VITALS section.
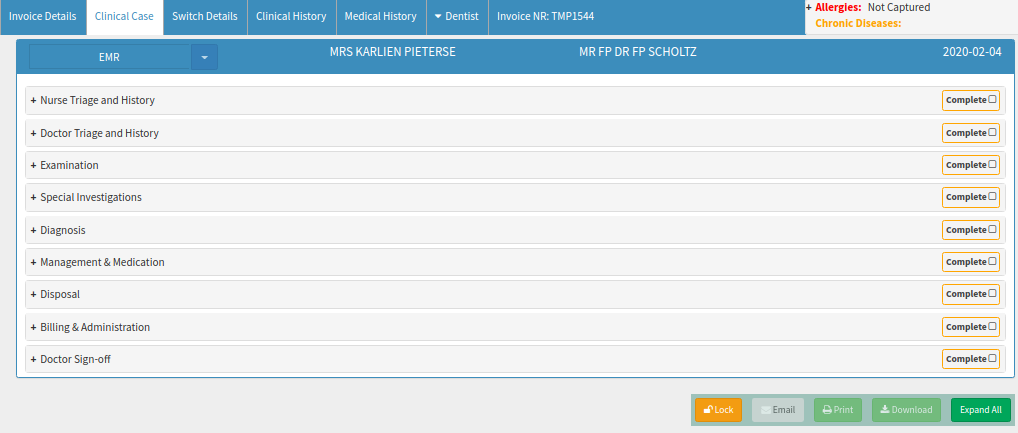
- Lifestyle: the Patients lifestyle habits can be selected here for example smoking, drinking or the use of any recreational drugs.
- Allergies: the Patient's allergies will be completed and saved under this section for the Doctor Vitals. This will affect scripting as a warning will display should you, for example, prescribe Amoxicillin to a patient that is allergic to penicillin.

- Examination: In the physical/medical examination, the doctor examines the patient for any possible medical signs or symptoms of a medical condition or accident. In this section, the Doctor can add images related to the illness or injury or mark the sketches provided after examining the Patient.

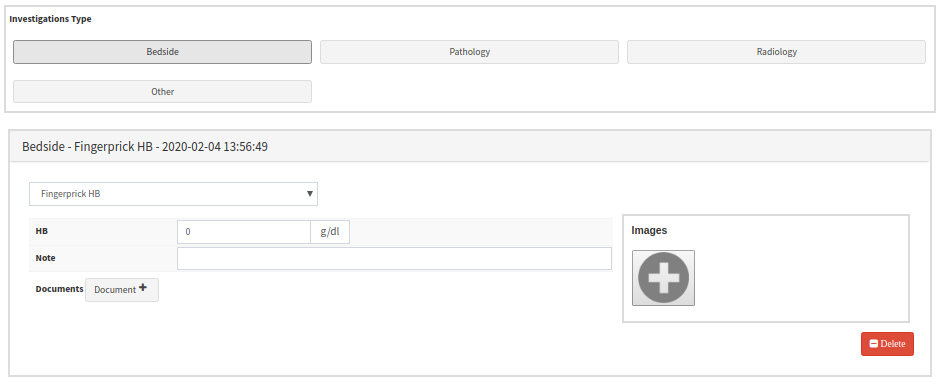
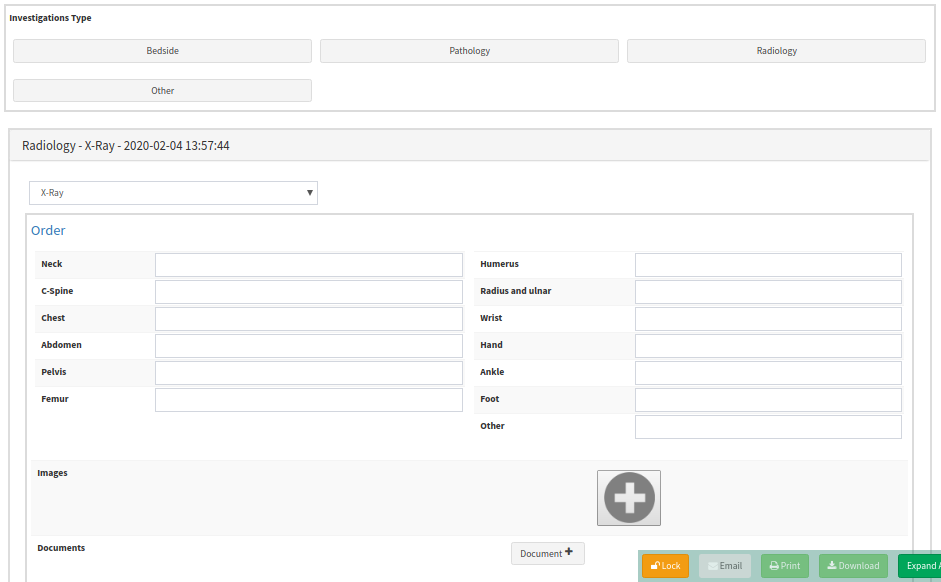
- Special Investigation: After the patient's vitals and physical examination were done the Doctor might send the patient for more tests to determine a diagnosis. In this section the Doctor can send the patient for blood works, x-rays or any other scans or tests required.

- Bedside - Fingerprick HB: Haemoglobin can be performed by the Doctor as a simple bedside test on a fingerprick sample of blood using a hand-held colour-comparison device.
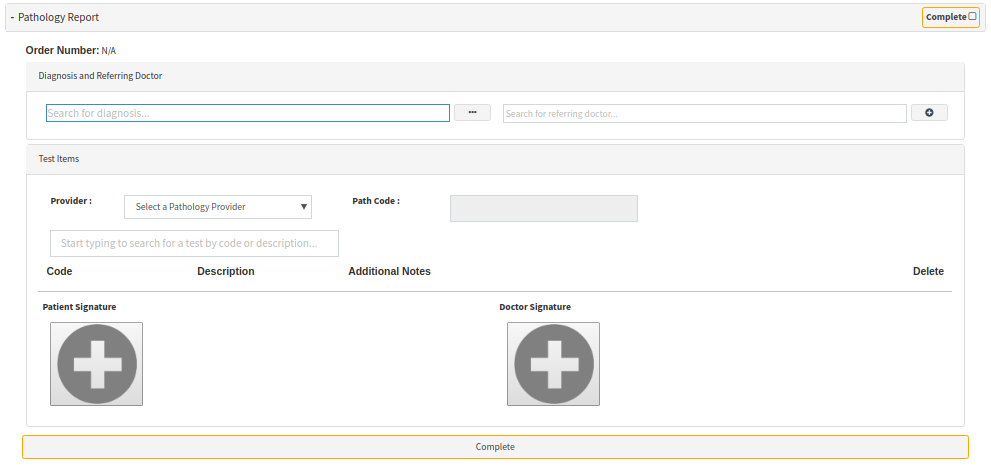
- Pathology Report: A pathology test is testing that examines your blood, urine or samples obtained by biopsy. Doctors will send the bloodwork to the Lab and use this information for diagnosis and treatment of diseases and other conditions.
- Radiology - X-Ray: An X-ray is a common imaging test that the Doctor will request in the ER if the patient was in an accident etc. It can help your doctor view the inside of your body without having to make an incision. This can help them diagnose, monitor, and treat many medical conditions. Different types of X-rays are used for different purposes.
- Ultrasound: is a medical test that uses high-frequency sound waves to capture the inside of a person's body. The human ear cannot hear this sound wave. The doctor can request for the patient to have a sonar done while in the ER to help him determine a diagnosis and treatment plan.


- Diagnosis: In this section, the Doctor will know and complete the diagnosis by identifying the nature of the patient's illness or other problems. He will complete the case type and case subtype and complete the ICD-10 code related to the diagnosis.
- EMR Case Types: the purpose of setting up the EMR Case Types is for the Practitioner to select under what category type the diagnosis or procedure falls, in the EMR Form under the Clinical event. The EMR Case Types can be set up in the Web App Settings >> Entity Settings >> Clinical Form Settings.

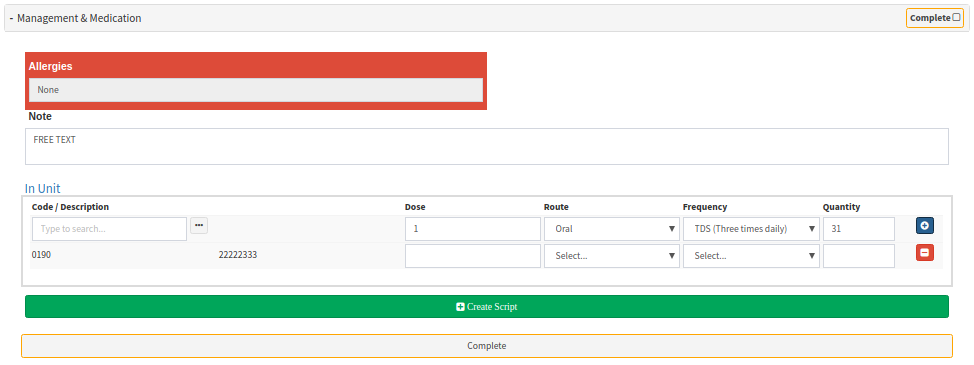
- Management and Medication: the purpose of this section is to help the Doctors and regulators to focus on mitigating the risks for medication management in the emergency room. Reducing opportunities for medication error and increasing the opportunities for a safe medication management environment represents a prime opportunity to improve the healthcare delivery system. You will complete and issue a script from here for the Patient.
- Disposal: In this section, you will complete what happened to the Patient while they were in the ER. Were they admitted to the Hospital, Discharged, Transferred to another facility, Died, etc. Under every option is a section that needs to be completed.

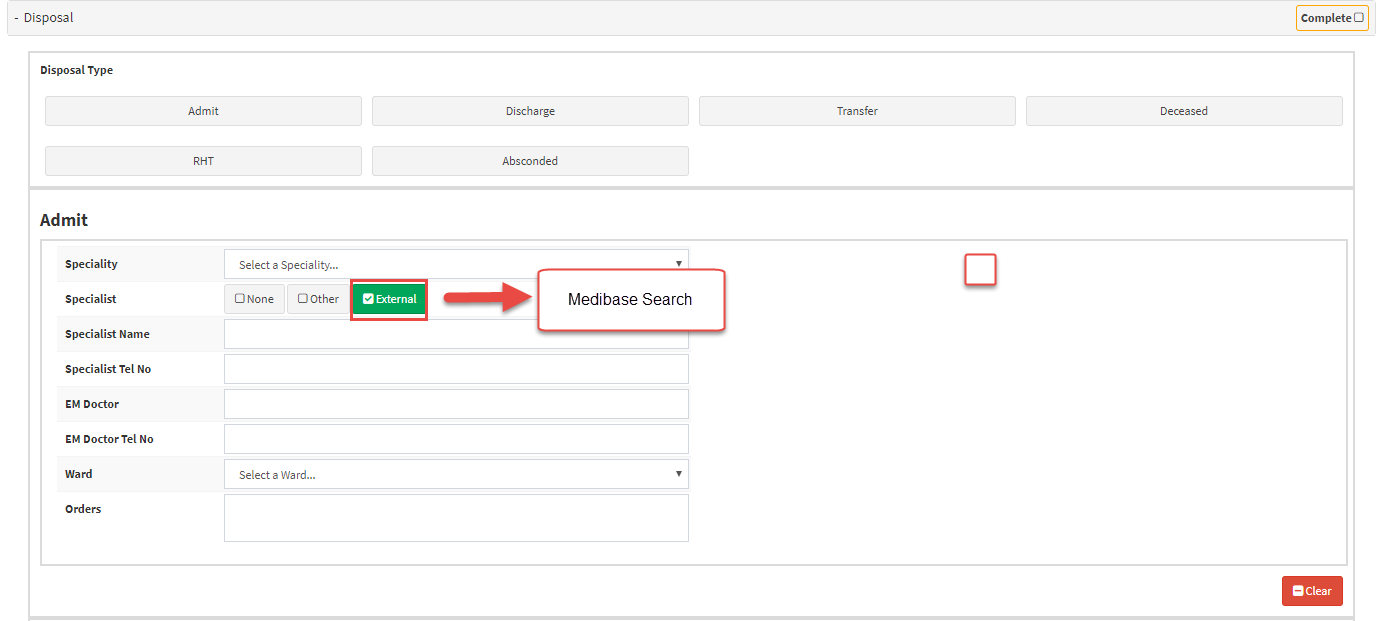
- Admit: The patient will be admitted to the Hospital in this section. All the hospital details will be completed here.
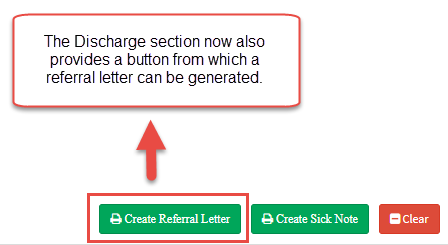
- External button: Select a debtor >> On the sidebar select Clinical >> Select a Form to Add >> EMR >> Disposal >> Admit / Discharge >> Transfer >> Select Search External >> A new search filter has been added to the EMR form, under the Disposal section, to connect to Medibase and handle all search operations >> The Discharge section now also provides a button from which a referral letter can be generated.
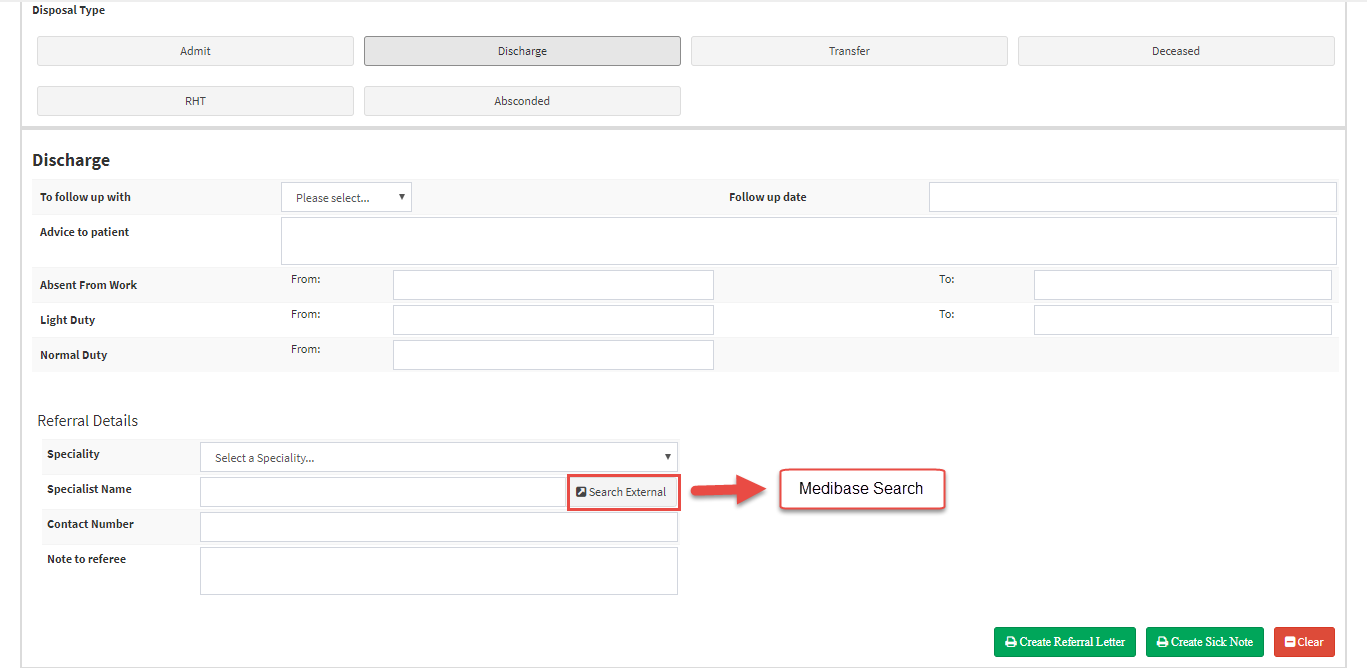
- Discharge: After the patient was treated and the Doctor said the Patient can go home the Patient will be discharged from the hospital or Emergency Room.
- You can create a Referral Letter and Sick Note from this section for the Patient.
- Transfer: If the patient needs to be transferred from the Emergency Room or Hospital to another facility the transfer section will be completed with the necessary information.
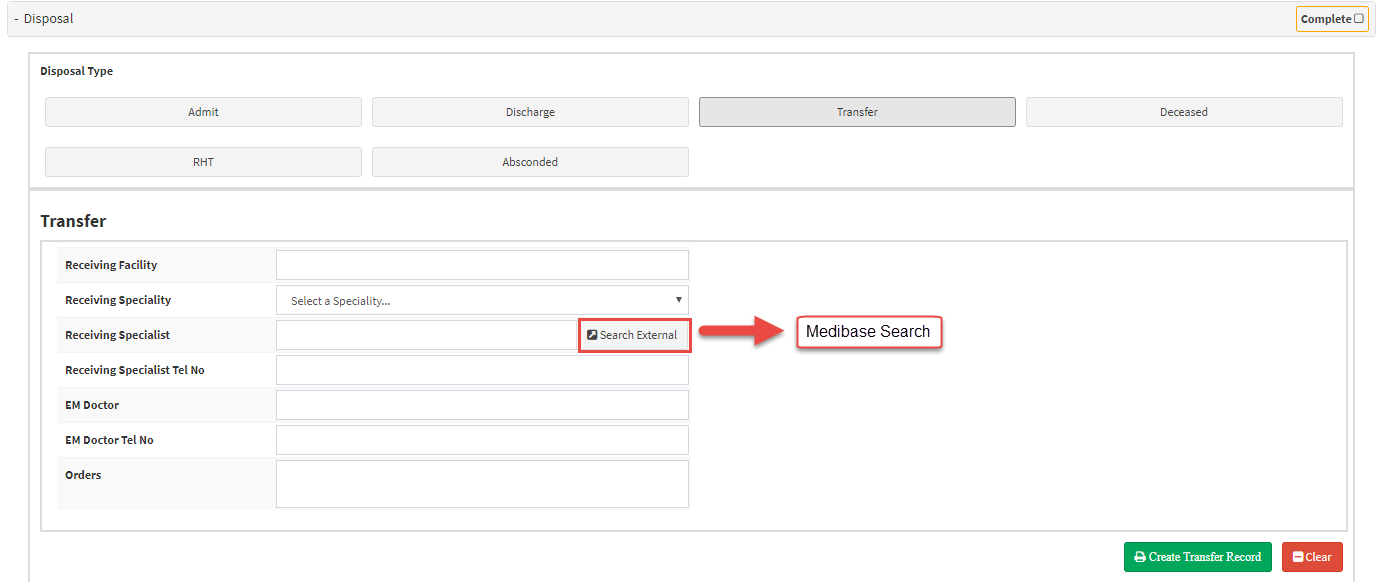
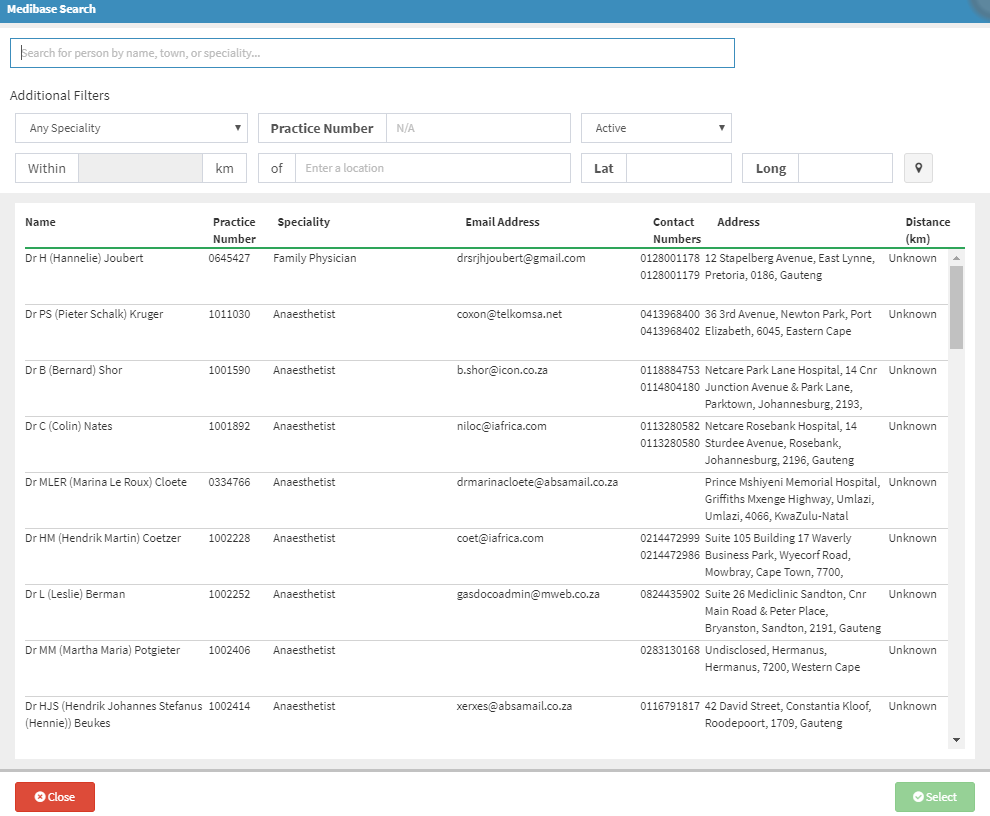
- Medibase Search: Medibase is the definitive source of healthcare contact information in GoodX. Medibase prides itself as the largest, most accurate, most complete and most up to date source of healthcare contact information available. The Online Directory is freely available to GoodX clients, for any and all healthcare information needs.
- Deceased: If the patient passed away the Doctor will complete this section.
- DOA: Death on Arrival
- DIU: Death In Unit

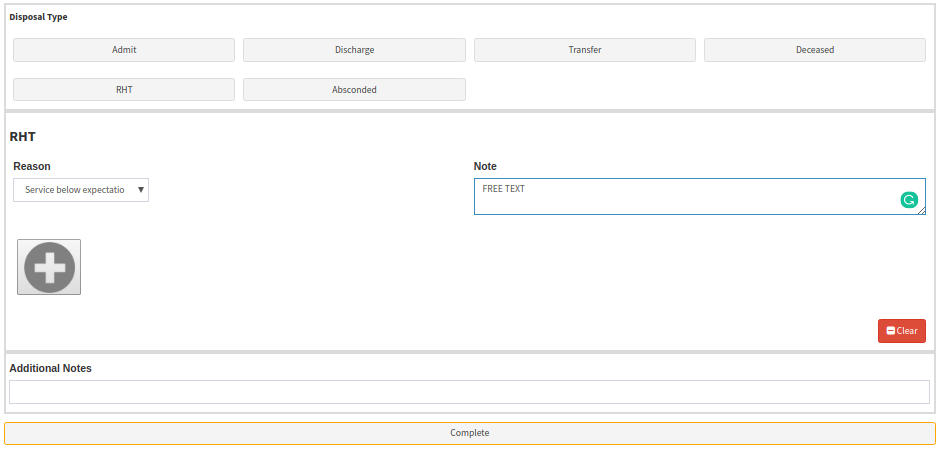
- RHT: Refusal of Health. If the patient was not examined or help and left the Doctor can complete this section and give a reason for the RHT.
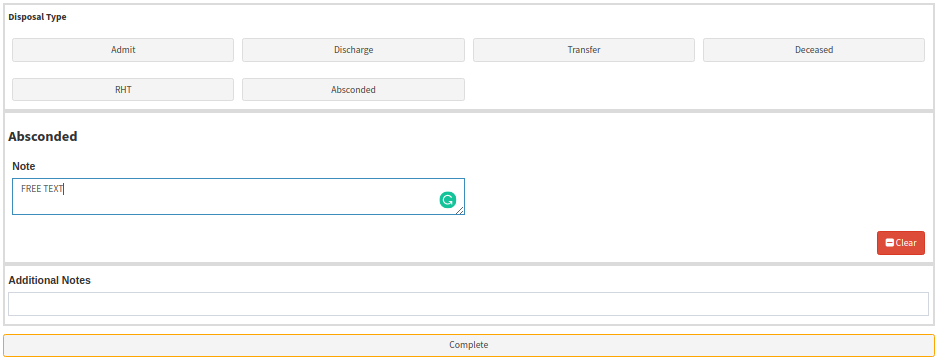
- Absconded: Refers to an instance where a patient in care in the Emergency Room or Hospital cannot be located within the treatment unit and that the patient's whereabouts are unknown. Free text section for the Doctor to make notes about the incident.
- Patient Handover: the doctor on call needs to capture certain information when a patient is handed over at the start of a new shift. The information needs to be captured in this (Disposal) section when the 'Patient Handover' box is ticked and should contain the following information from the Dr handing over the patient:
- Date and Time: Date and Time of the Handover - the date and time will default to the current date and time on the system automatically but can be edited by the user.
- Handover To: Details of the doctor that will continue with the treatment of the patient - this field is a searchable input field allowing the user to search for a treating doctor from the Treating Doctor List in GoodX. You can search by Title and Surname and select the Dr from the list.
- Note: Notes made by the doctor that is handing over the patient - this is a free text area where the user can type a handover note. They can include any notes and important detail regarding the patient prognosis and treatment up to the point of handover.

- Billing and Administration: In this section, the billing for the consultation and procedures will be done after the Doctor has discharged the patient from the ER. It will either be submitted to Medical Aid or the Patient will settle the account then and there before leaving the emergency room.


Take Note: When any of the ward visits are selected in the Doctor Triage and History and this section is 'Completed' a billing code, specific to the type of visit, will automatically be added to the Billing and Administration section of the EMR. This billing code will be flagged with a red A, as is the current case with all billing codes that are automatically added in other parts of the EMR.
Only when the user marks the Doctor Triage and History as Completed/Finalized will the appropriate billing code (as seen below) be added automatically. The following billing code will be added in accordance with the type of Hospital visit selected:
- Ward – will add 0109
- High Care – will add 1204
- ICU – will add 1210

- Doctor Sign-Off: The Doctor will add his signature to the EMR Form after every section was completed.
- Click on Complete when you've completed all the Sections.
TAKE NOTE: Remember to click on Save and Close to save all the changes.
