Text size
Line height
Text spacing
Workflow Event Templates are used to standardise and streamline the creation of common clinical and administrative events within the system. By using predefined Workflow Event templates, you can save time, reduce manual entry errors, and ensure consistency across departments. These templates help you maintain accurate records, improve communication, and support efficient Patient care by making sure the right information is captured in the right format every time.
💡Please Note: Only Workflow Events with available User Guides are listed. Please contact your FCL or designated support person if you require documentation on a Workflow Event that has not been listed.
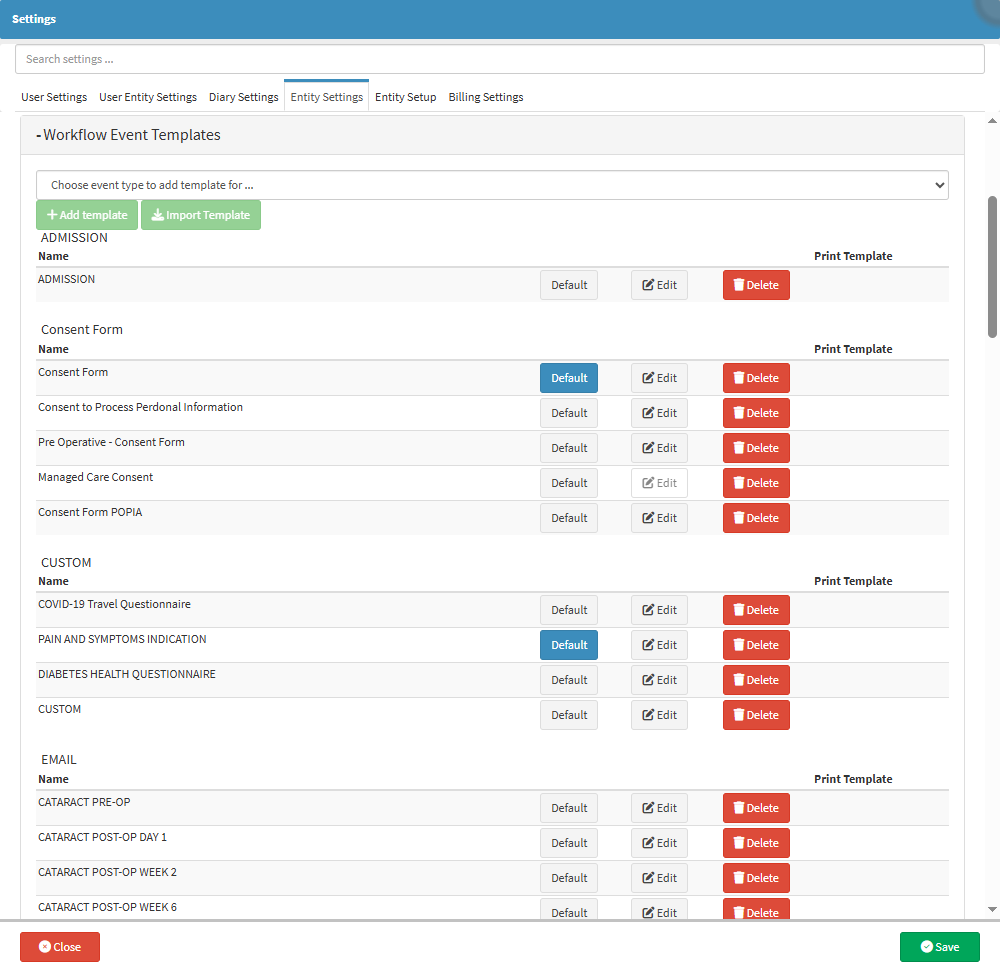
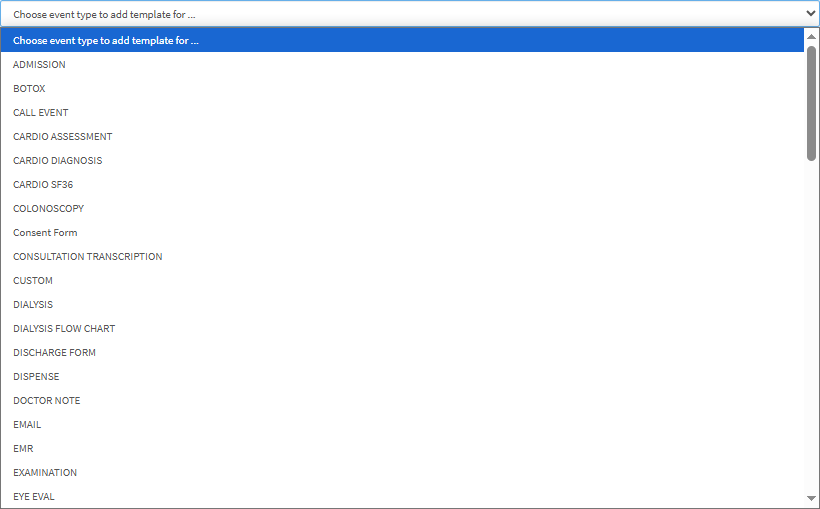
An explanation of templates with available User Guides will be given in alphabetical order:
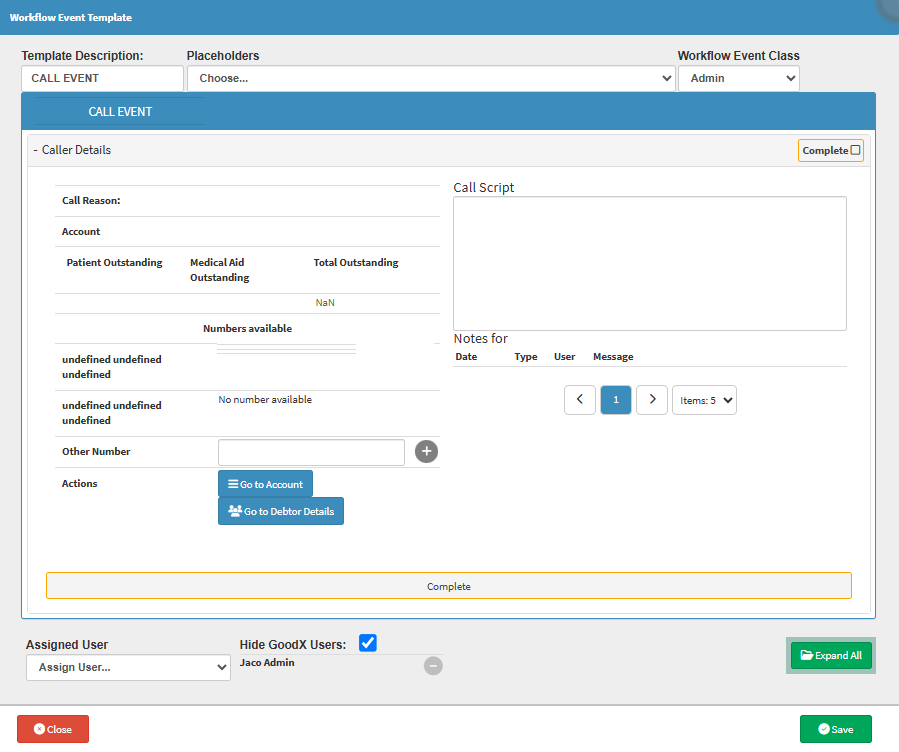
The Call Event template allows you to tailor call documentation to specific needs, whether it’s billing follow-ups, appointment reminders, or treatment discussions. By capturing only the relevant information during each call, the workflow becomes more efficient, ensuring important details aren’t missed. It also standardises how calls are recorded, which supports accountability, accurate record-keeping, and clear communication between team members.
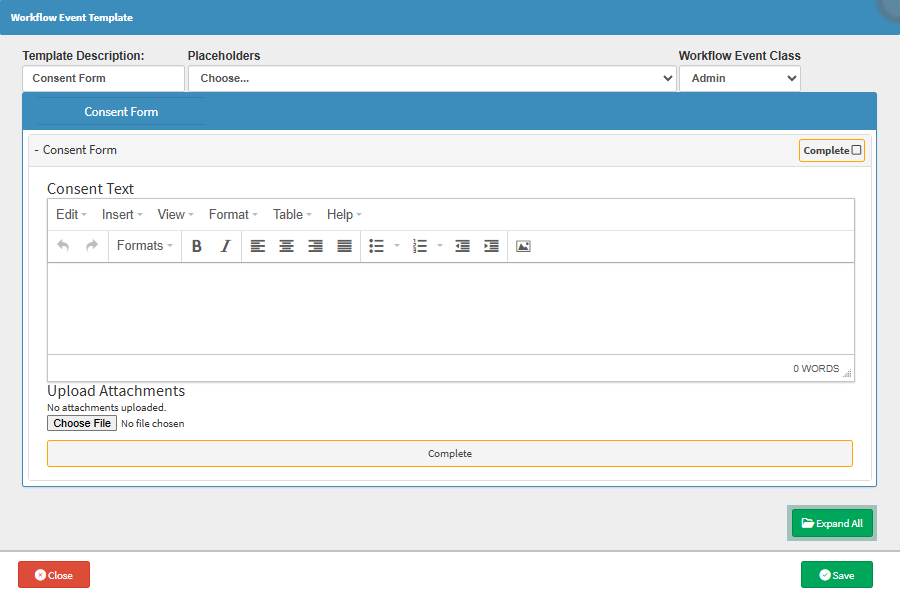
The Consent Form template ensures that the language, content, and structure of the form can be adapted to suit different procedures, legal requirements, or Patient profiles. This flexibility helps Practitioners communicate procedure-specific risks and obtain informed consent in a way that is both legally sound and easy for Patients to understand. It also supports consistency in documentation while allowing for necessary medical or legal customisation, reducing the risk of misunderstandings and improving overall compliance.
The Custom template allows you to create forms with custom questions that are tailored specifically to the preferences of the Practitioner's needs. It is possible to add questions containing drop-down menus, checkboxes, radio buttons, etc. You can also add scoring to each question that allows them to make conclusions based on the answers received.

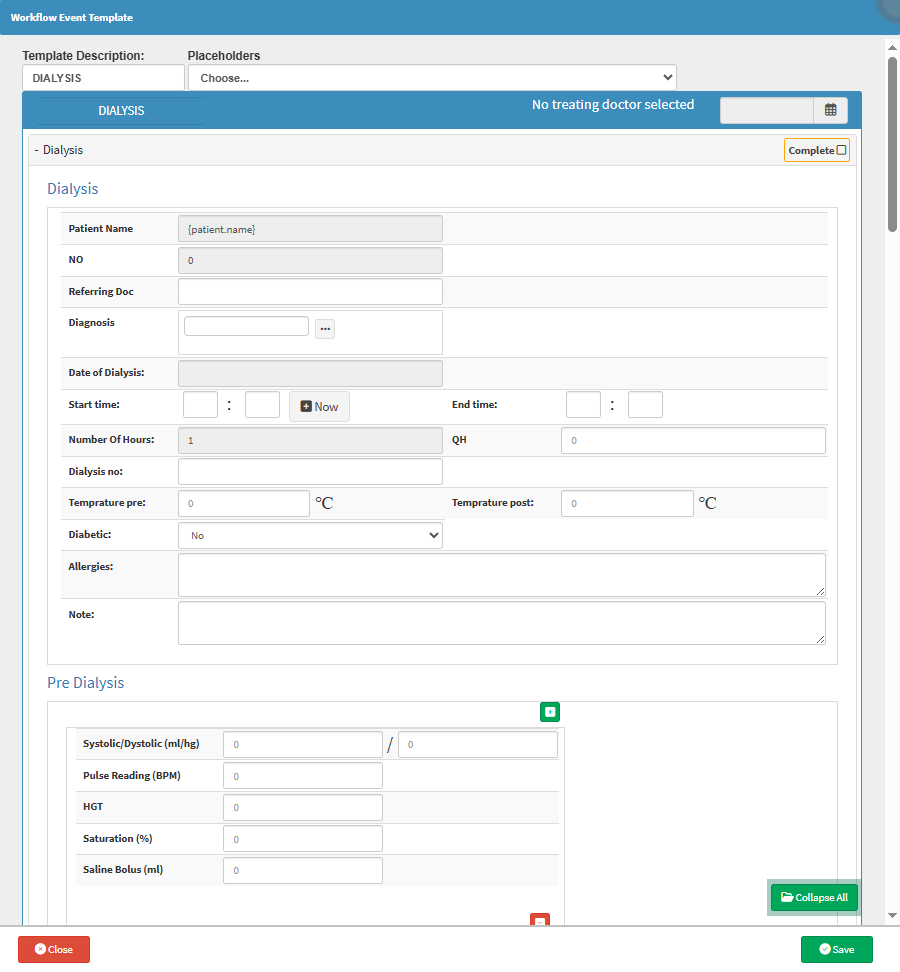
The Dialysis template allows you to efficiently capture and track all relevant clinical details for each dialysis session, such as fluid balance, vitals, medications administered, and session outcomes. This ensures consistent documentation, supports continuity of care, and helps monitor the Patient’s response to treatment over time.
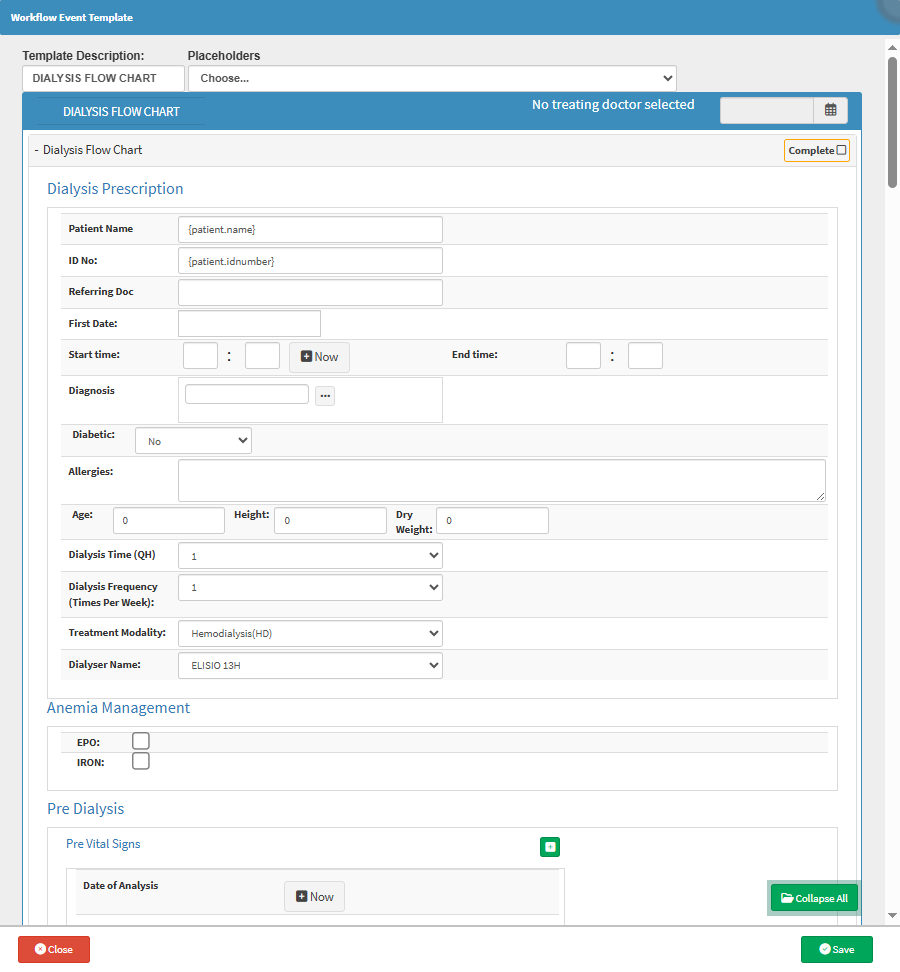
The Dialysis Flow Chart template allows you to document and monitor the dialysis process in a structured, time-based format. It helps track key metrics such as blood pressure, fluid removal, and machine settings throughout the session. This ensures accurate, real-time recording, supports clinical decision-making, and provides a clear visual reference for ongoing Patient management.
The Discharge Form template is used when a Patient is ready to go home, is transferred to another facility or, in the case of death, to formally discharge them from the bed. It records the admission and discharge times, refusal of treatment (if applicable), follow-up details, and any relevant notes.

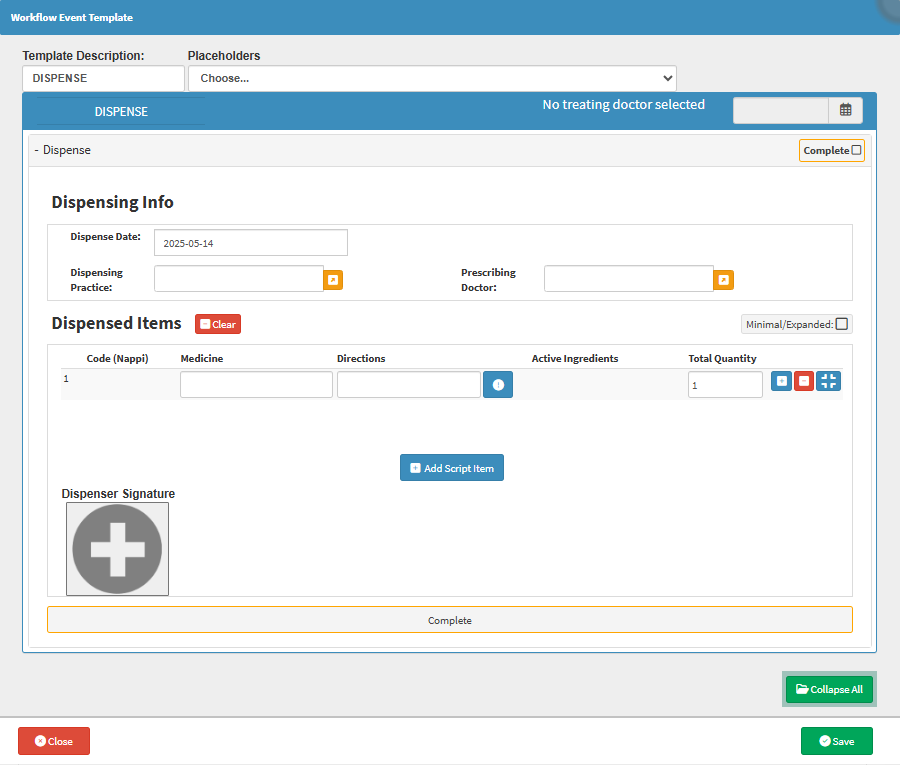
The Dispense template is a form that the Practitioner will use to dispense medication to a Patient and allows the Pharmacist or responsible person to dispense the items to the Patient from within the Practice instead of issuing a prescription that the Patient will have filled at an external Pharmacy.
The Doctor Note template allows each healthcare provider to tailor the note format to their specific workflow, clinical focus, or speciality. This ensures that all relevant information, whether clinical observations, lab results, or treatment decisions, is captured in a structured, consistent manner. It reduces the risk of critical details being missed, supports better collaboration across care teams, and improves the accuracy of ongoing medical records and reporting. 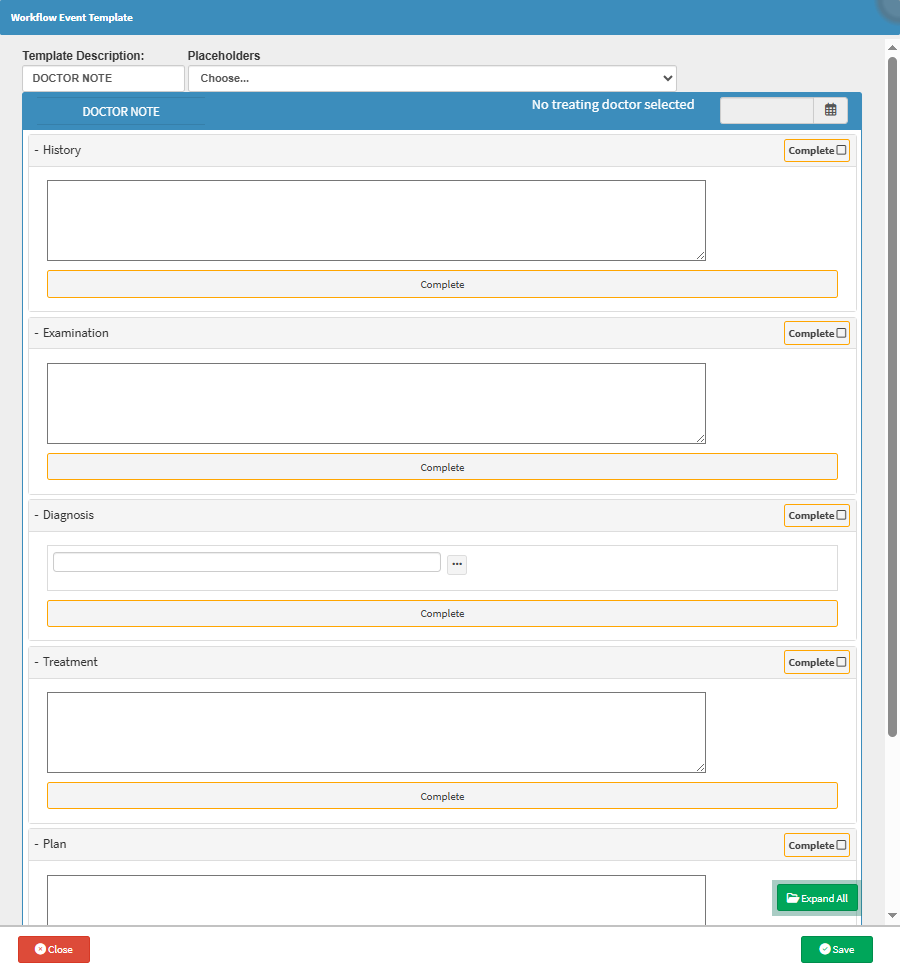
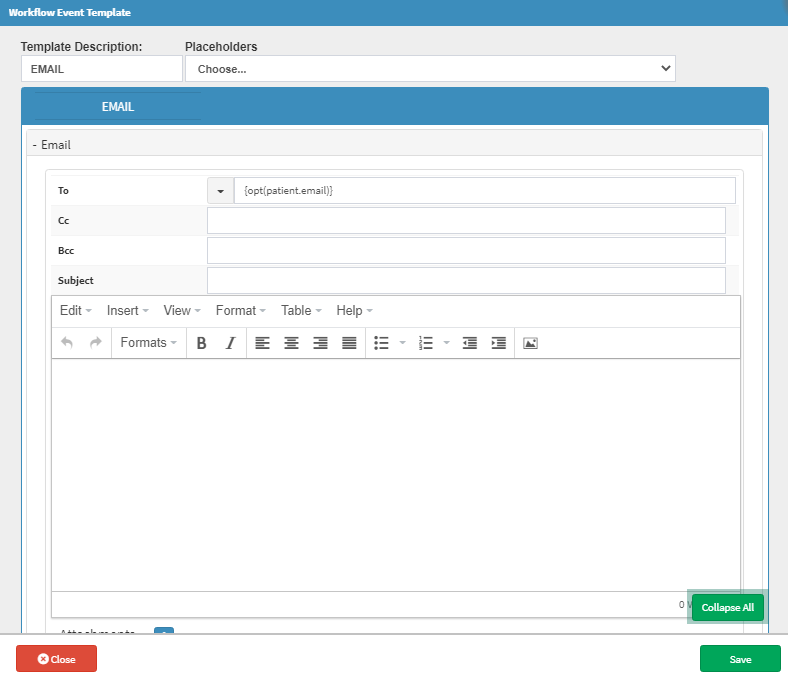
The Email template ensures that messages are consistently worded, professionally formatted, and relevant to the recipient, whether it’s a Patient, Debtor, or another Practitioner. It saves time, reduces manual errors, and ensures compliance by including all necessary information automatically. Templates can also be tailored to suit different communication needs, like sending Sick Notes, Invoices, or lab results, making every interaction smooth and efficient.
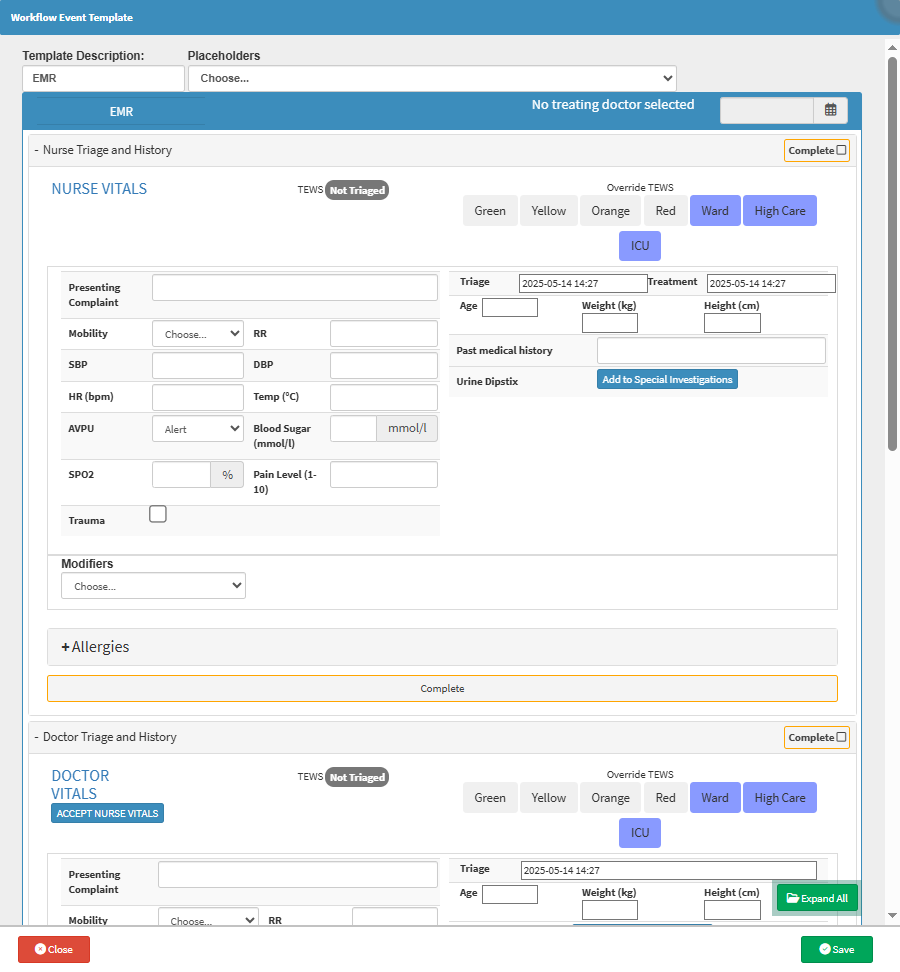
The EMR template ensures that vital information, such as the Patient’s medical history and vital signs, is captured quickly and consistently in emergencies. It streamlines communication between nursing staff and Practitioners, reduces duplication of effort, and allows for faster clinical decision-making. With the key details already documented, the Practitioner can immediately focus on assessing the Patient and determining the appropriate treatment, saving valuable time when it matters most.
The Examination template provides you with the ability to customise an Examination form according to the specific needs and focus areas of your Practice. This customisation ensures that only relevant fields and options are included in the form. The structured layout of the Examination form is designed to facilitate quick and efficient capture of a Practitioner's observations. 
The Eye Eval template is used to document the results of various eye tests performed by the Practitioner. It allows for visual annotations on provided diagrams and supports image uploads from external sources. As the form is completed, billing codes are automatically added, enabling the Practitioner to bill the Patient seamlessly during the assessment.

The Eye Eval 2 template allows you to tailor the form to suit their specific clinical approach and preferences. This flexibility supports the capture of more accurate and relevant data, improves efficiency during assessments, and enhances the quality of documentation. With built-in drawing tools, image upload functionality, and automatic billing integration, the template streamlines both clinical and administrative workflows, making it easier to provide focused care while saving time.

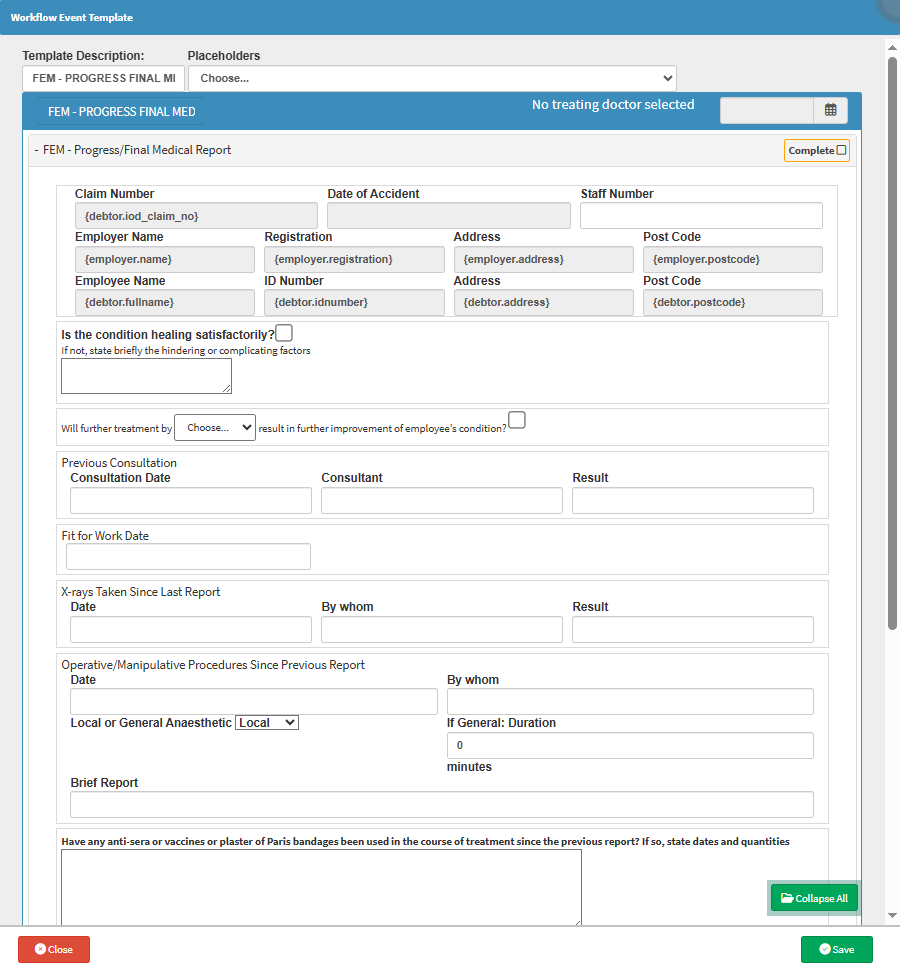
The FEM - First Medical Report template ensures that all required incident, medical, and treatment details are captured accurately and in line with specific regulatory or organisational requirements. It allows Practitioners to adapt the form to include relevant fields for different types of injuries or occupational illnesses, improving clarity and reducing administrative back-and-forth. This not only supports faster claims processing and legal compliance but also helps assess the Patient’s ability to return to work with precision and confidence.
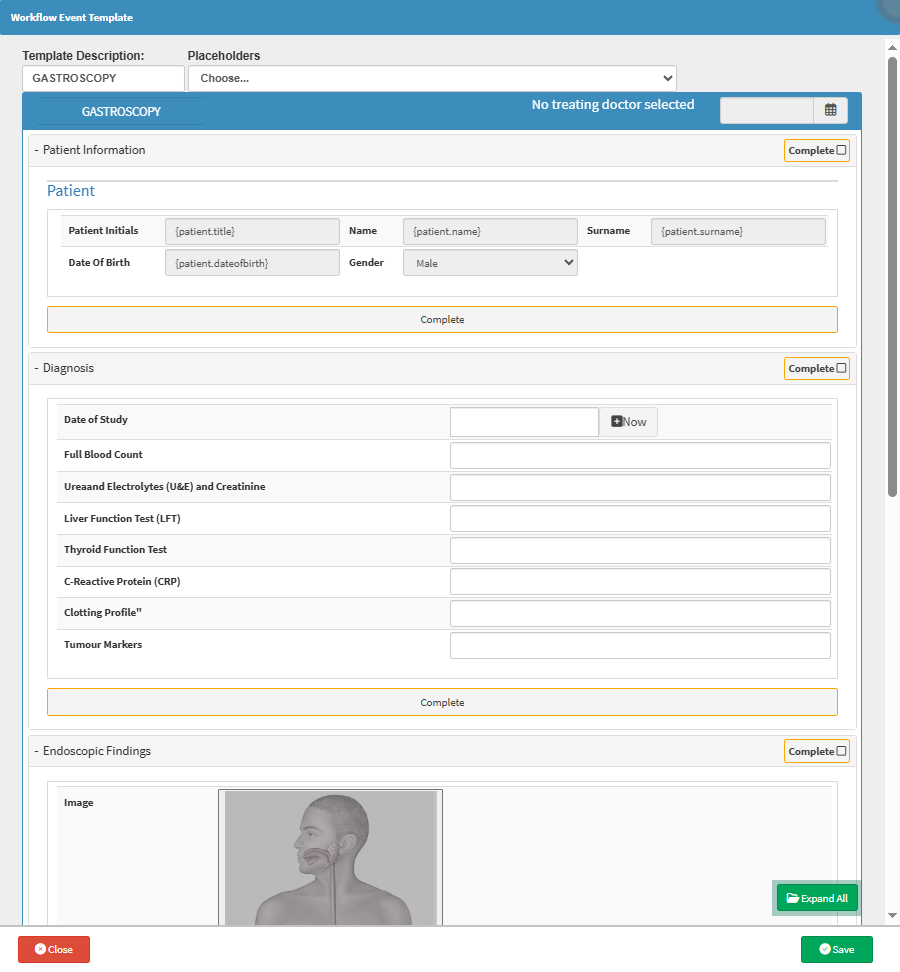
The Gastroscopy template allows you to tailor the form to the specific procedural preferences, reporting styles, and clinical needs of the Practice. It ensures that all relevant details, such as scope findings, biopsy sites, and complications, are captured accurately and efficiently. Custom fields can also be added for specific protocols or hospital requirements, improving consistency, saving time, and enhancing the quality of medical documentation and follow-up care.
The General Examination template allows you to adapt the form to suit different specialities, consultation styles, and Patient needs. It ensures that only relevant information is captured, reducing clutter and improving efficiency during consultations. Custom fields can highlight specific health risks, chronic conditions, or practice-specific protocols, resulting in more focused assessments, better clinical decisions, and improved continuity of care.

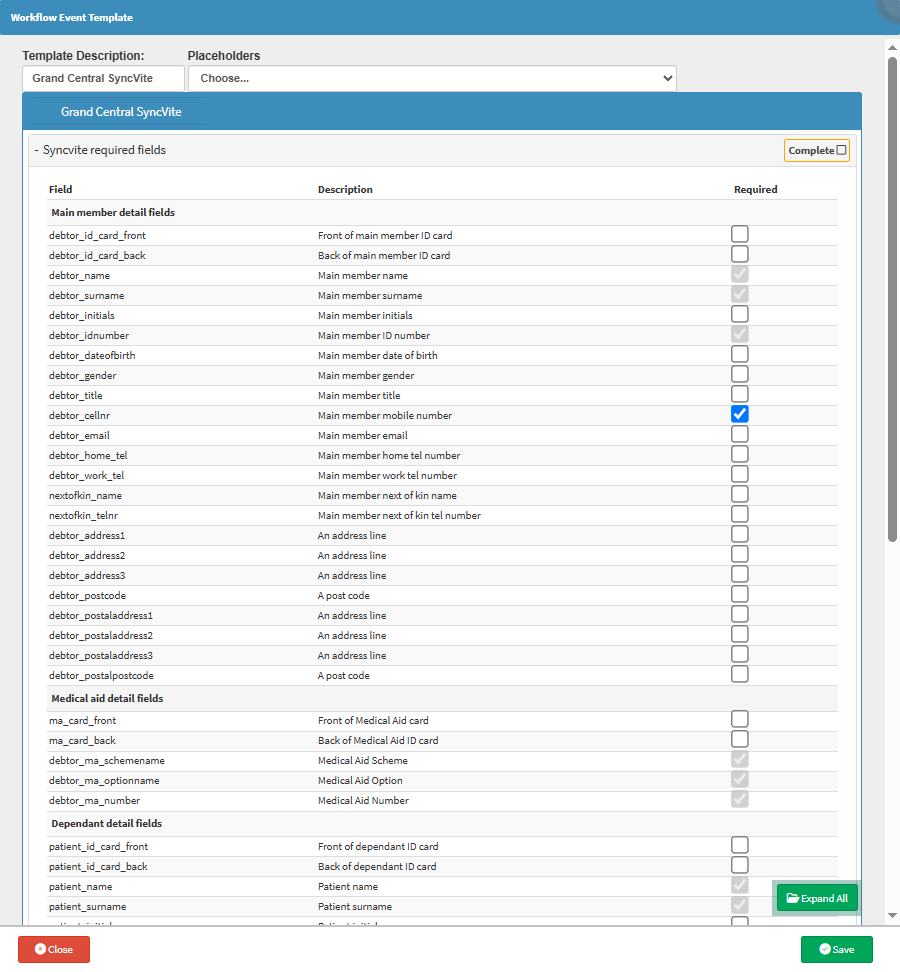
The Grand Central SyncVite template allows the Practice to tailor the invitation content to suit their communication style, branding, and specific information requirements. It ensures clarity in what is being requested from the Patient, improves response rates, and enhances data accuracy. By customising which fields are editable or required, the practice can streamline the process of collecting or updating Debtor demographic data, reducing admin time, minimising errors, and maintaining a clean, up-to-date database for smoother patient interactions and billing processes.
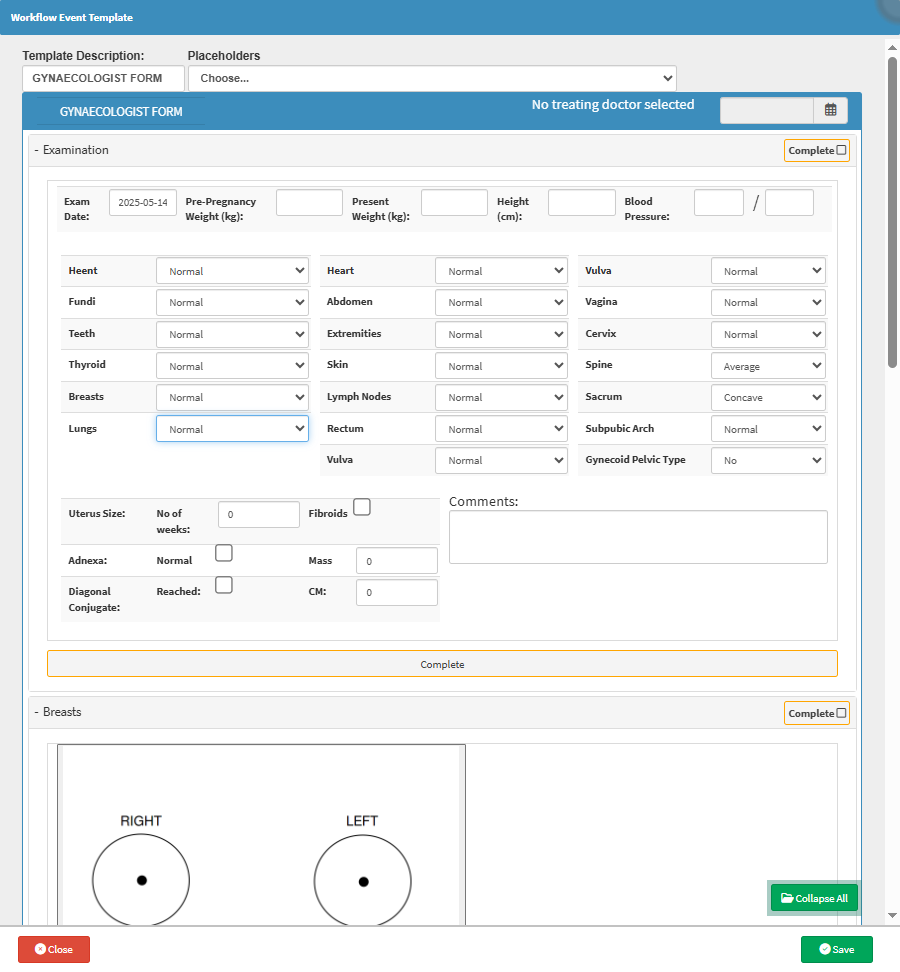
The Gynaecologist Form template allows you to tailor the form to different procedures, appointment types, or patient needs. Whether it’s for routine pelvic exams, prenatal check-ups, or post-operative follow-ups, the form can be adjusted to capture only the most relevant clinical details. This flexibility improves the accuracy and clarity of documentation, supports personalised care, and ensures compliance with medical and legal standards while also streamlining the billing and reporting process.
The Letter template allows you to set up letters that they can use to seamlessly integrate examination information into a letter specifically designed for referral purposes. The information will automatically populate all the relevant information onto the form. This allows for the efficient inclusion of relevant details from the examination, ensuring comprehensive and accurate communication when referring a Patient to another Healthcare Professional or Specialist. Using the Letter streamlines your referral process and eliminates the need for duplicate work. 
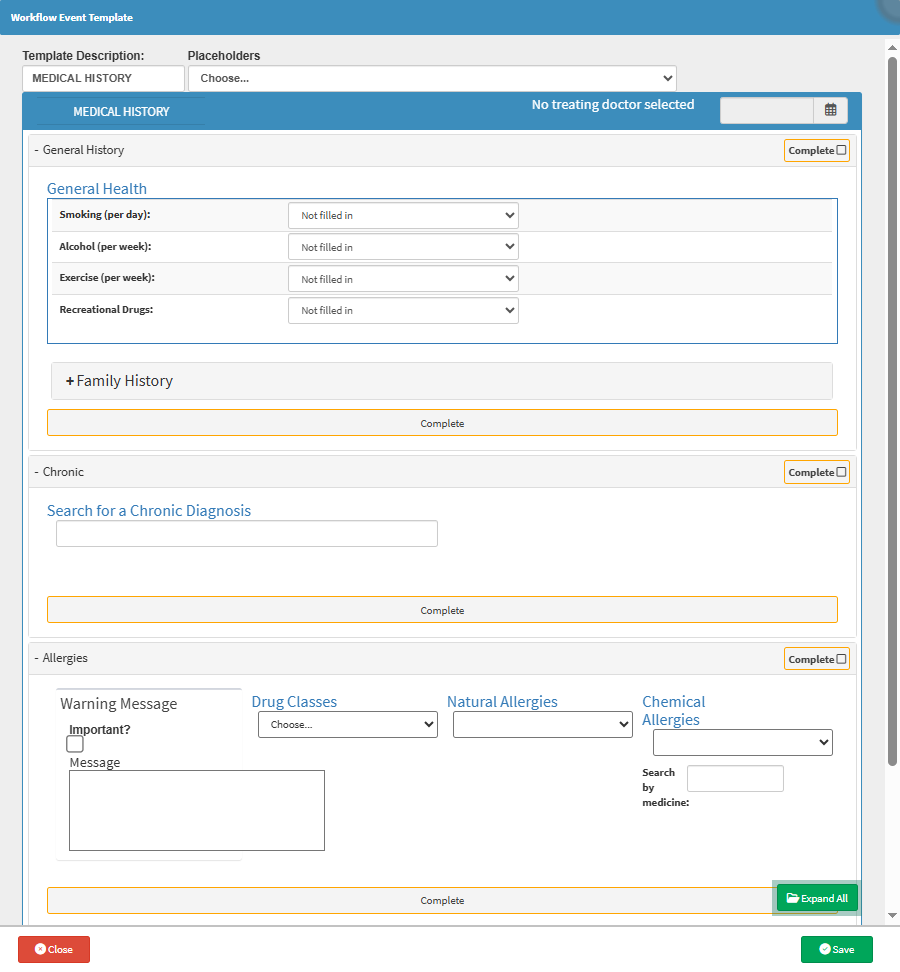
The Medical History template allows you to tailor the form to capture relevant personal and family health details specific to their speciality or practice needs. This ensures critical information is recorded consistently and thoroughly, improving diagnosis accuracy and personalised treatment plans. Custom fields can highlight hereditary risks or condition-specific history, helping streamline clinical assessments and supporting better long-term care.
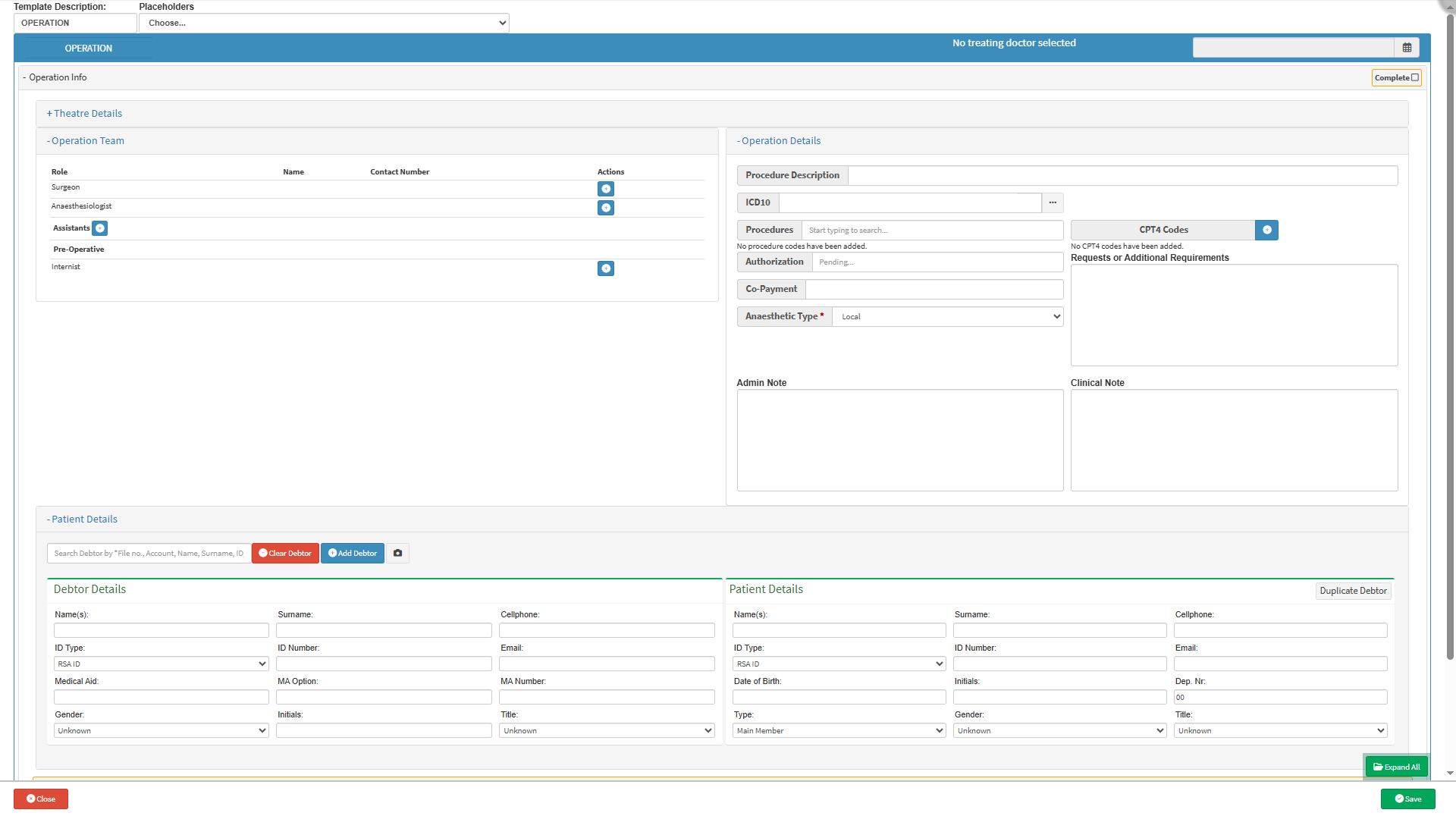
The Operation template allows you to tailor the documentation to specific surgical procedures, hospital protocols, and individual preferences. This flexibility ensures all critical details, such as operative findings, anaesthesia, are accurately recorded. It also includes the names and contact details of the Surgeon, Anaesthesiologist, and Assistants, ensuring clear communication and accountability throughout the surgical process. Custom fields support compliance with legal requirements, streamline billing processes, and help maintain a comprehensive medical record that supports quality patient care and future reference. Integration with theatre scheduling and imaging systems further enhances workflow efficiency.
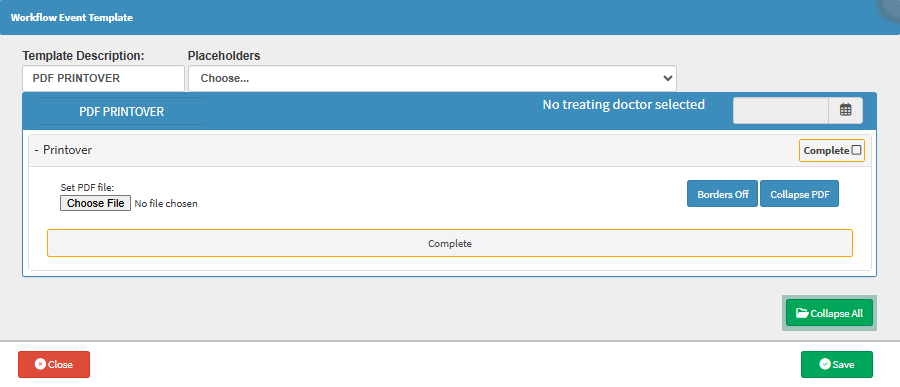
To use the PDF Printover form, the setup first needs to be done. Once set up, the PDF Printover template lets the practice automate the filling of various forms like PMB Registration or Medical Aid Registration with accurate patient data tailored to specific requirements. This saves time, reduces manual errors, and ensures forms are consistently completed to standard. Customisation means the template can be adapted as forms or regulations change, keeping processes smooth and compliant without the usual paperwork headaches.
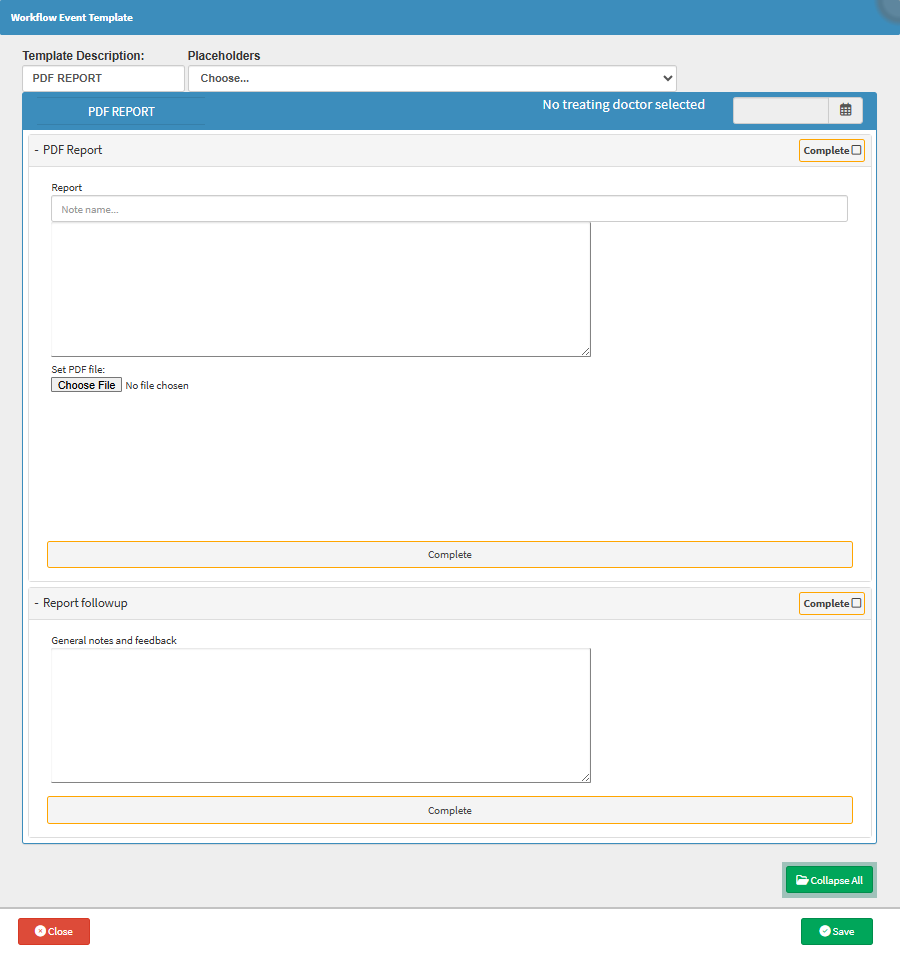
The PDF Report template enables you to tailor document uploads to specific workflows, ensuring consistent formatting and metadata for easier retrieval. This flexibility supports quick organisation of referral letters, test results, and other documents, making them instantly accessible and system-compatible. Customisation improves efficiency, reduces errors, and helps maintain a clean, well-structured patient record for seamless clinical use.
The Physio Assessment template allows you to tailor the form to capture all necessary details specific to their treatment approach and patient needs. This ensures accurate, thorough documentation of medical history, diagnosis, and treatment plans, supporting better clinical decisions. It also helps flag when a patient needs referral for further medical evaluation, improving patient safety and care continuity, all while streamlining record-keeping and reducing admin hassle.

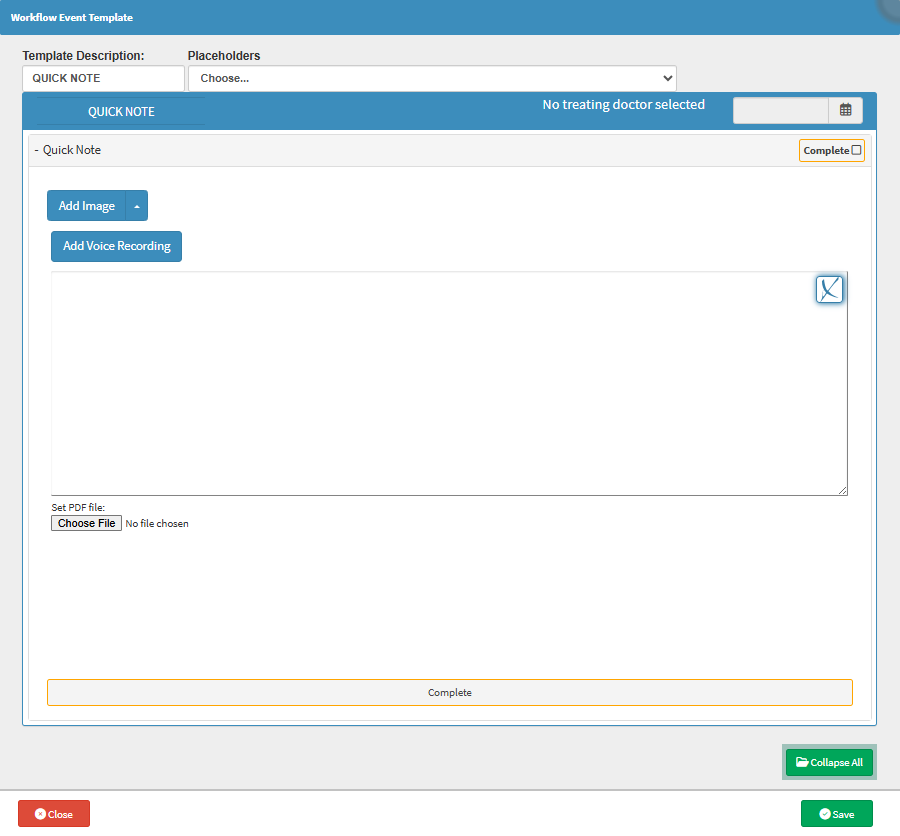
The Quick Note template allows you to capture key info and images exactly how they need to, whether it’s for quick updates, observations, or reminders. Tailoring the template means notes are organised, relevant, and easy to find later, boosting continuity of care and making follow-ups way smoother. Plus, it cuts down on time wasted hunting for details, so clinical decisions get made faster and smarter.
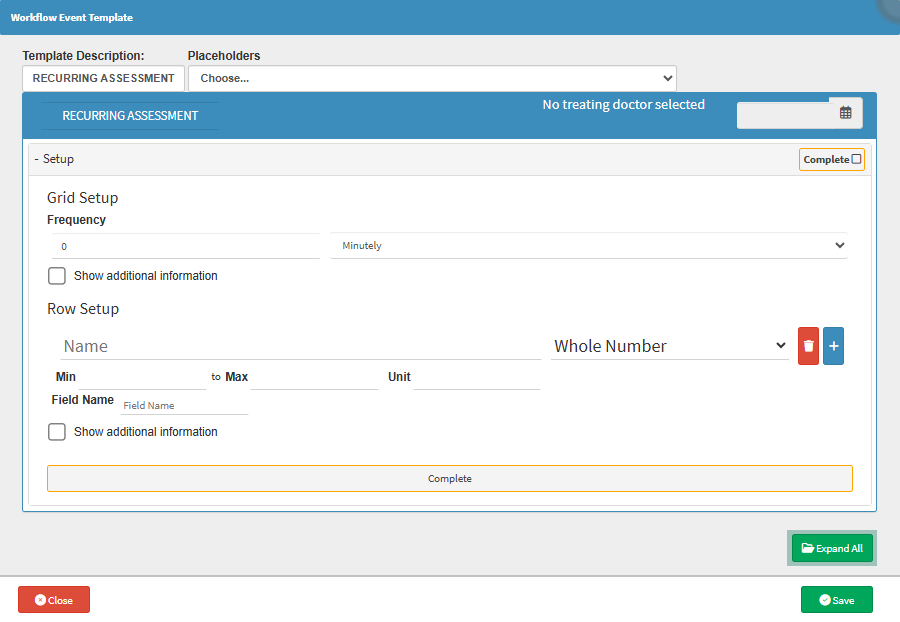
The Recurring Assessment template allows you to tailor evaluation criteria and schedules to each Patient’s unique care plan. This ensures consistent tracking of progress over time, helping spot trends or issues early. Customisation supports better clinical decisions, improves treatment quality, and reduces admin by automating reminders and documentation, all while keeping care personalised and on point.
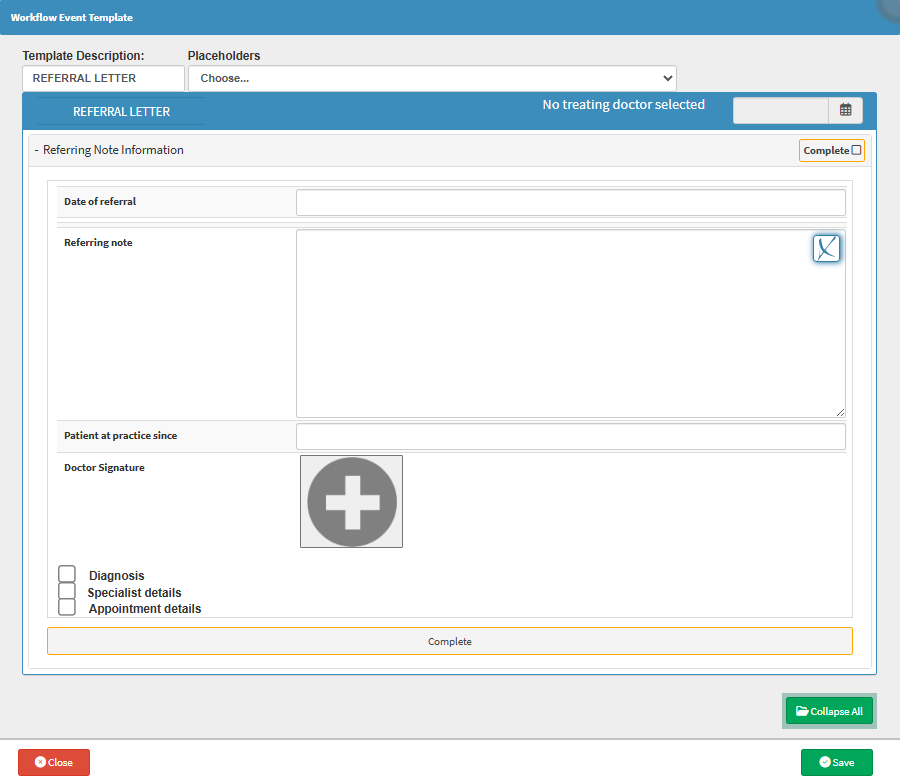
The Referral Letter template allows you to tailor the letter to the specific needs of the Patient and the receiving Specialist. This ensures all relevant medical history, examination findings, and reasons for referral are documented, promoting seamless communication and continuity of care. Customisation saves time by auto-populating key details while allowing flexibility for personalised notes, improving professionalism and efficiency in patient management.
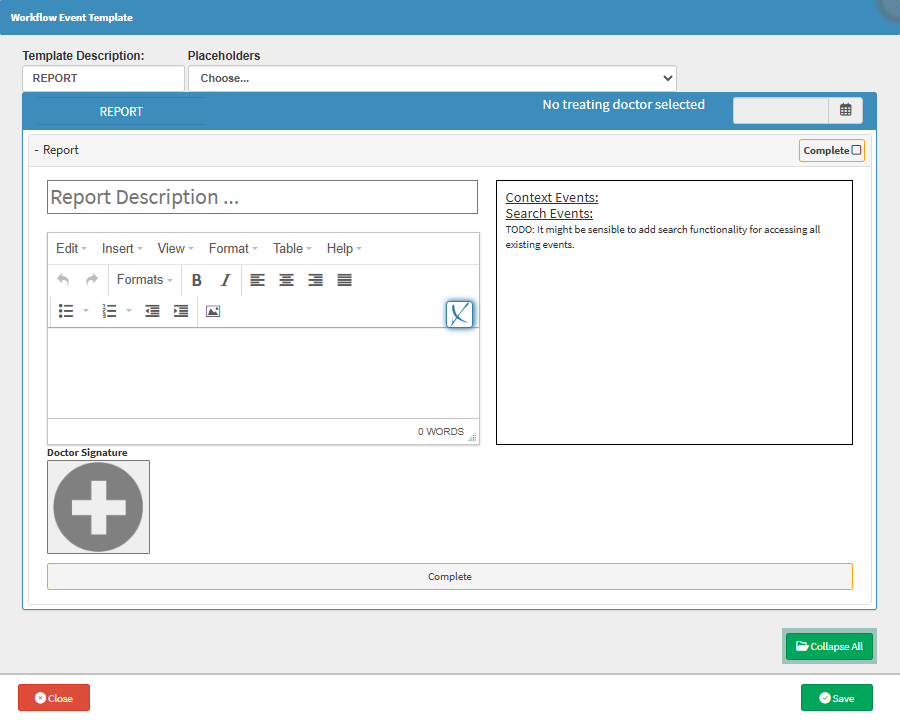
The Report template lets Practitioners tailor how they capture and present crucial clinical or administrative info, whether it’s exam findings, test results, treatment plans, or procedural summaries. This flexibility ensures reports are clear, comprehensive, and relevant to specific cases, boosting communication between healthcare teams and supporting faster, smarter medical decisions. Plus, it helps keep documentation legally solid and audit-ready without drowning in paperwork.
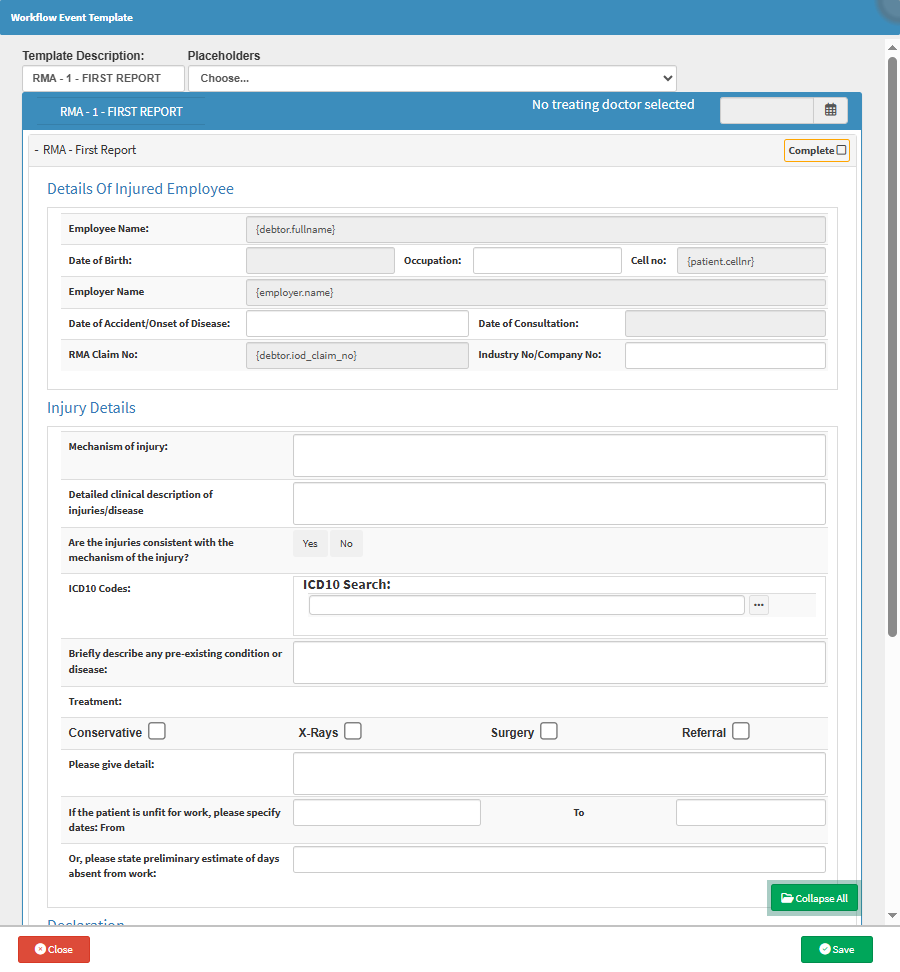
The RMA-1 - First Report template ensures that all required medical and claim-related information is captured accurately and consistently. It helps the Practitioner complete the report efficiently, reduces the risk of missing critical details, and speeds up the claim verification and submission process. This not only improves compliance with regulatory requirements but also supports faster outcomes for both the Patient and the medical practice.
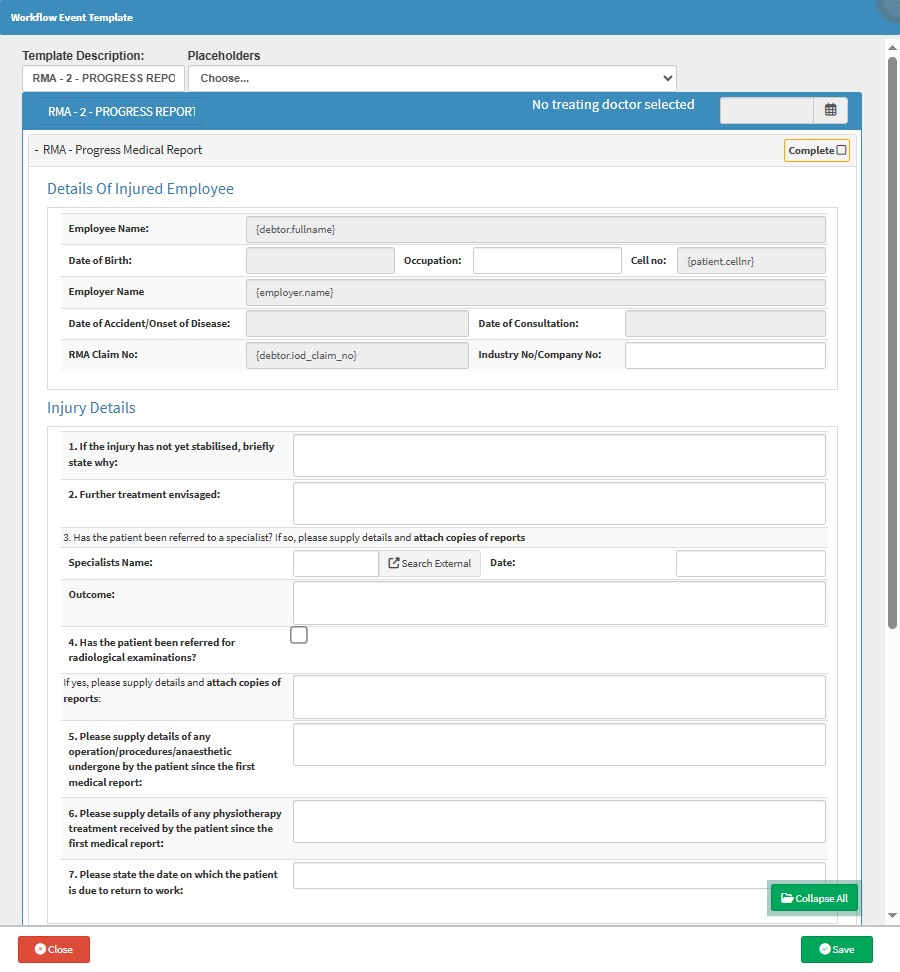
The RMA-2 - Progress Report template ensures that follow-up details after an Injury on Duty (IOD) consultation are consistently and accurately recorded. Practitioners can adapt the layout to match specific reporting requirements, include only the relevant clinical updates, and streamline how tests, treatments, and recovery progress are tracked. This not only saves time but also ensures compliance, improves claim accuracy, and strengthens communication between Healthcare Providers, Insurers, and Employers.
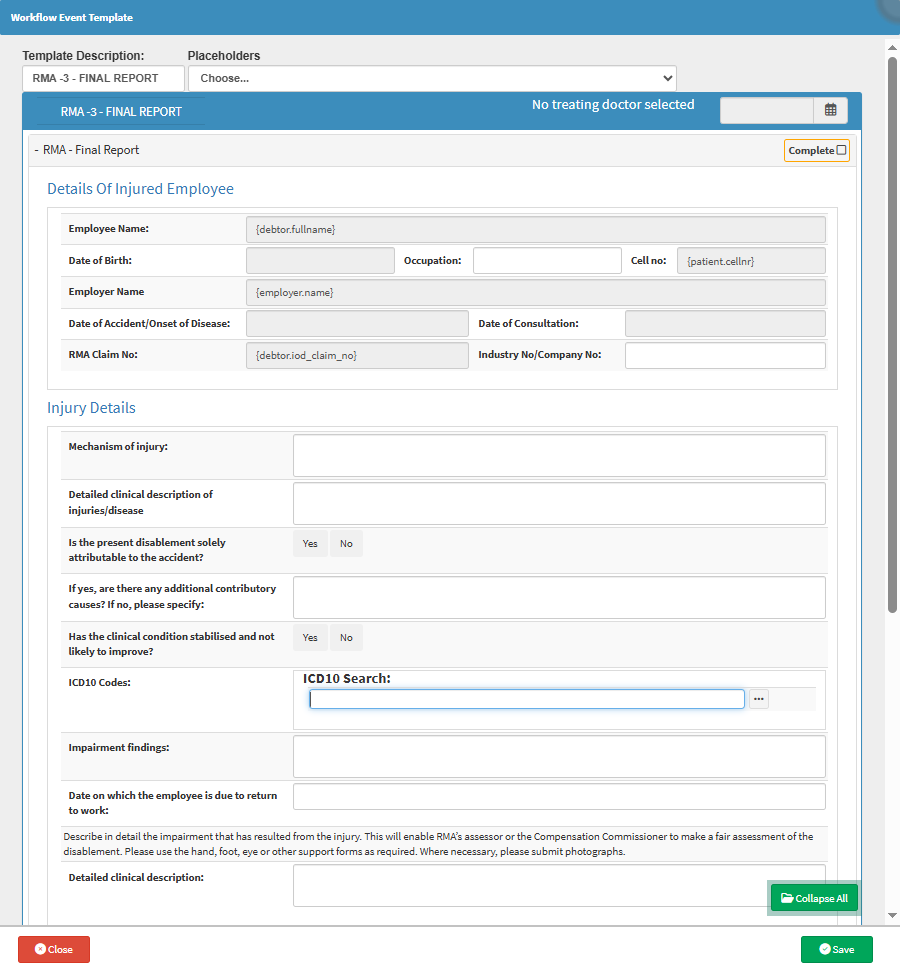
The RMA-3 - Final Report template allows you to accurately summarise the outcome of the Patient’s treatment journey after an Injury on Duty (IOD). With flexibility to tailor the format, they can clearly outline medical conclusions, permanent impairments, if any, and whether further intervention is needed. This supports faster claim processing, ensures legal and medical compliance, and provides a clean, complete record for both the Employer and Insurer. Custom fields also reduce errors and make the report feel less like paperwork and more like progress.
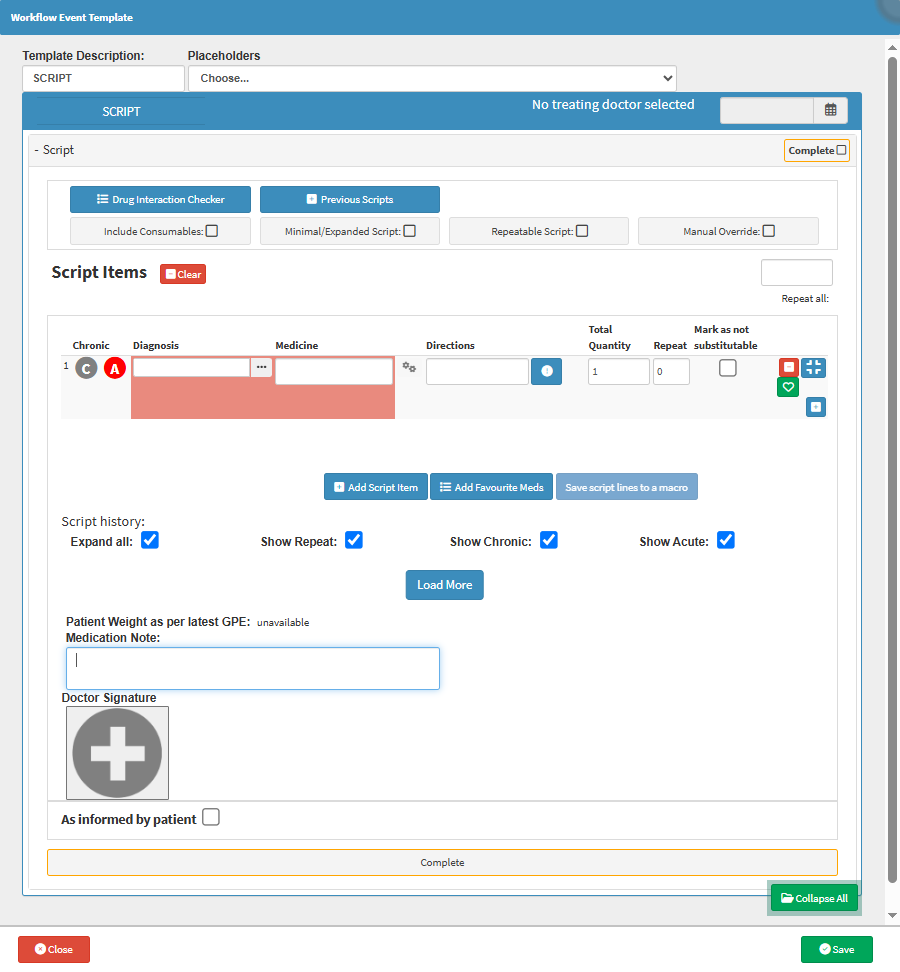
The Script template ensures that you can quickly and accurately prescribe long-term Medication tailored to each Patient’s ongoing condition. It allows the inclusion of repeat instructions, specific dosage schedules, and notes relevant to the Patient’s treatment plan. By standardising the format while allowing flexibility, it reduces prescribing errors, speeds up the process, and ensures that Pharmacies receive all the necessary information. Plus, it supports better medication adherence and continuity of care.
The Sick Note template allows you to efficiently generate accurate, professional medical certificates tailored to each Patient’s condition and situation. It ensures consistency in documentation while allowing flexibility for specific instructions like fitness to return to work, travel clearance, or restricted duties. This not only saves time but also helps reduce errors, maintain compliance with workplace and legal standards, and improve communication between Practitioner, Patient, and Employer or School.

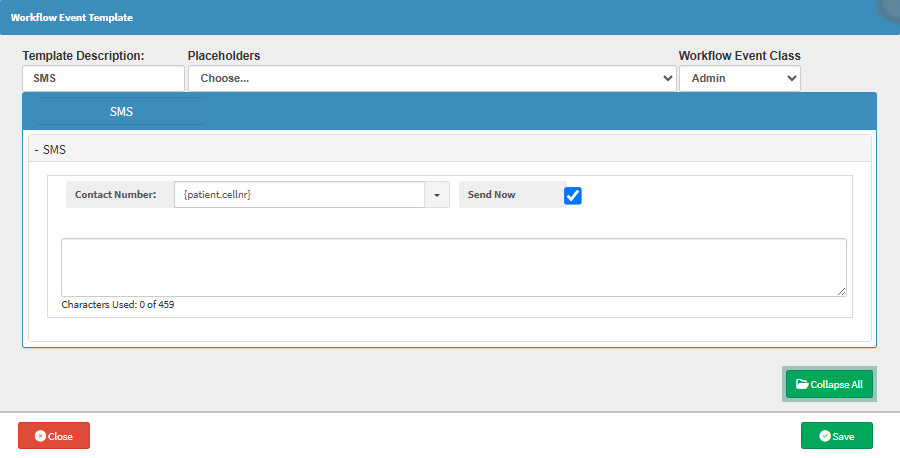
The SMS template allows Practitioners and admin staff to tailor messages for different scenarios like appointment reminders, payment alerts, or follow-ups, while keeping the tone professional and the content accurate. Instead of typing the same message over and over, risking typos or inconsistency, you can send clear, relevant communication with just a few clicks. It saves time, boosts efficiency and confidence in the Practice by being consistent.
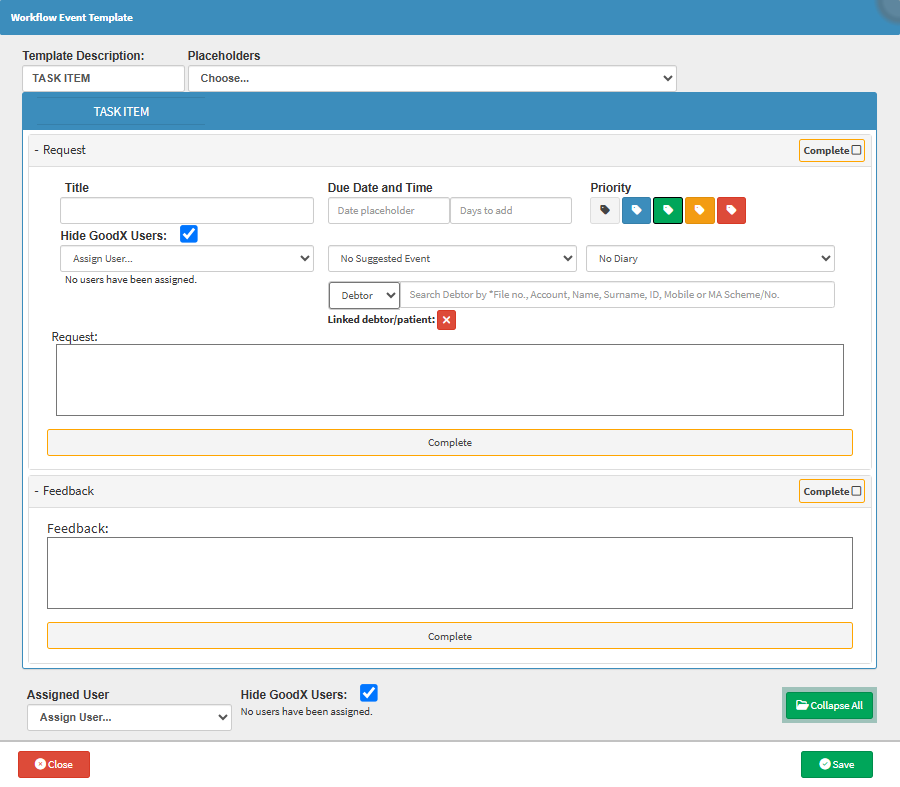
This template allows you to standardise how tasks are assigned, tracked, and prioritised, tailoring fields like deadlines, categories, or task types to match the Practice's workflow. This reduces miscommunication, ensures accountability, and speeds up delegation. Whether you're assigning routine follow-ups or urgent to-dos, having a consistent format keeps everyone focused and aligned.
The Telemed template ensures that every remote consultation captures consistent and relevant medical information tailored to the practice’s needs. It allows Practitioners to log symptoms, treatment plans, and patient concerns efficiently, while also including billing codes, consent notes, and follow-up actions. This not only saves time during virtual consultations but also ensures clinical and legal compliance, making remote care just as effective and professional as in-person consultations.
The Triage template allows emergency departments to tailor the form to match their protocols and workflows, whether it's for paediatrics, trauma cases, or routine ER visits. It ensures vital signs, presenting symptoms, and urgency levels are captured quickly and accurately. Auto-assigned urgency colours help fast-track critical patients, while custom fields can adapt to changing hospital needs or health crises. It boosts efficiency, accuracy, and patient safety when seconds count.

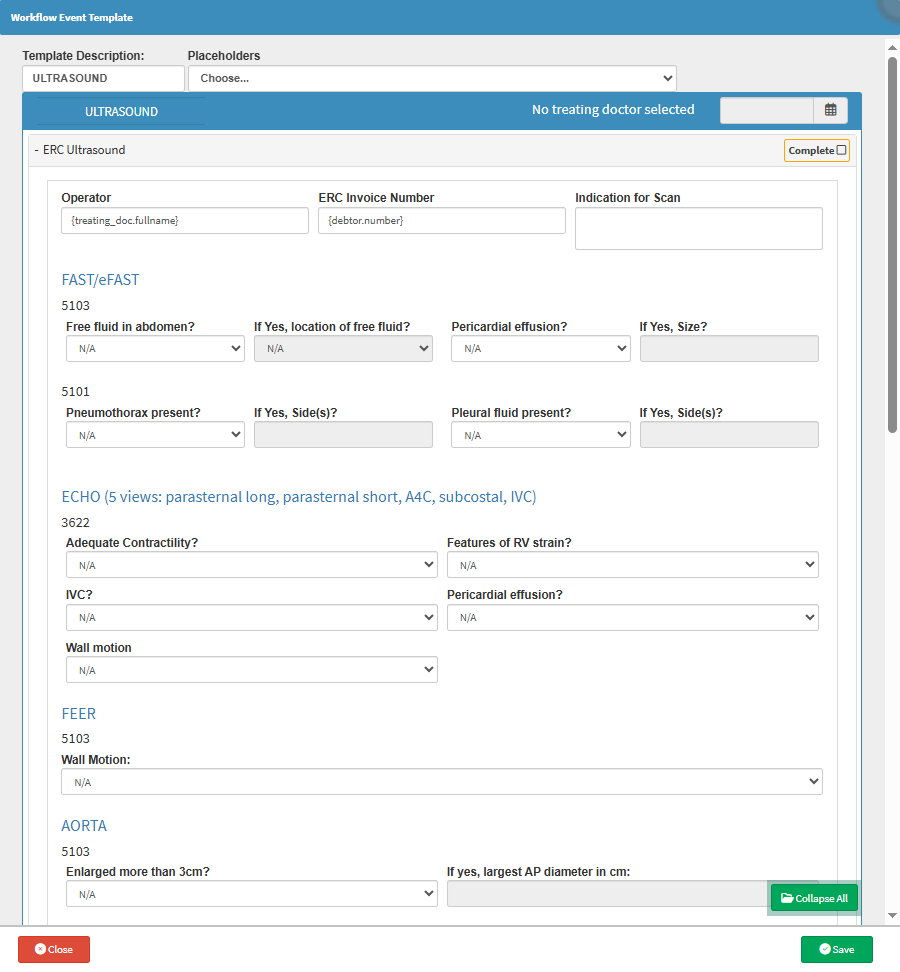
The Ultrasound template allows you to document findings consistently across different types of scans, whether abdominal, pelvic, vascular, or obstetric. It can be tailored to include specific measurement fields, image annotations, and diagnostic comments relevant to the body part or clinical question. Customisation ensures nothing important gets missed, supports faster reporting, and keeps everything standardised for audits, referrals, and follow-ups.
The WCA - Disease First Report template ensures that all legally required and medically relevant information is captured accurately and consistently when reporting workplace-related diseases or injuries. It allows Practitioners to tailor fields to specific types of incidents or industries, including condition-specific checklists, auto-fill patient data, and attach necessary supporting documentation. This reduces admin time, minimises the risk of incomplete submissions, ensures compliance with Workman’s Compensation Fund regulations, and speeds up claim processing.

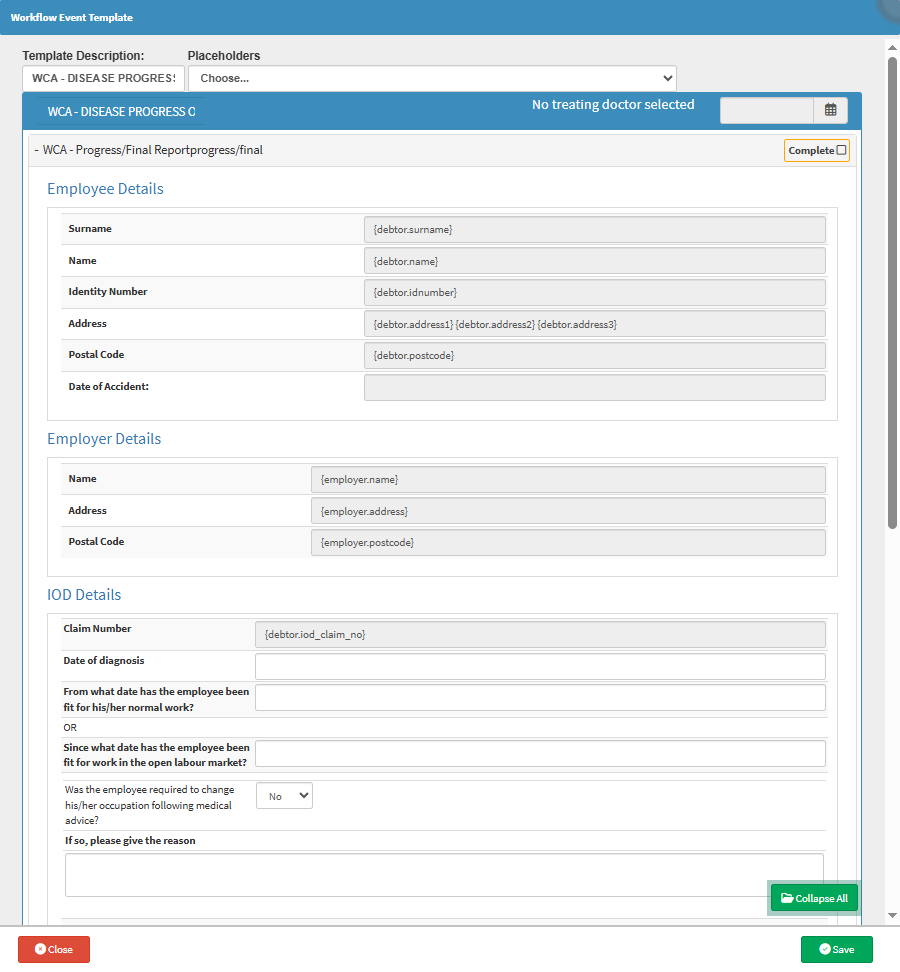
The WCA - Disease Progress Report or Final Report template allows you to document each stage of the Patient’s recovery with precision, based on the evolving clinical picture. Custom fields can be tailored to suit the nature of the occupational disease, track functional capacity over time, and note any workplace adjustments or job changes required. This supports accurate reporting to the Workman’s Compensation Fund, ensures continuity of care, and provides legal and medical clarity on whether the Employee can safely return to work or if a new role needs to be considered.
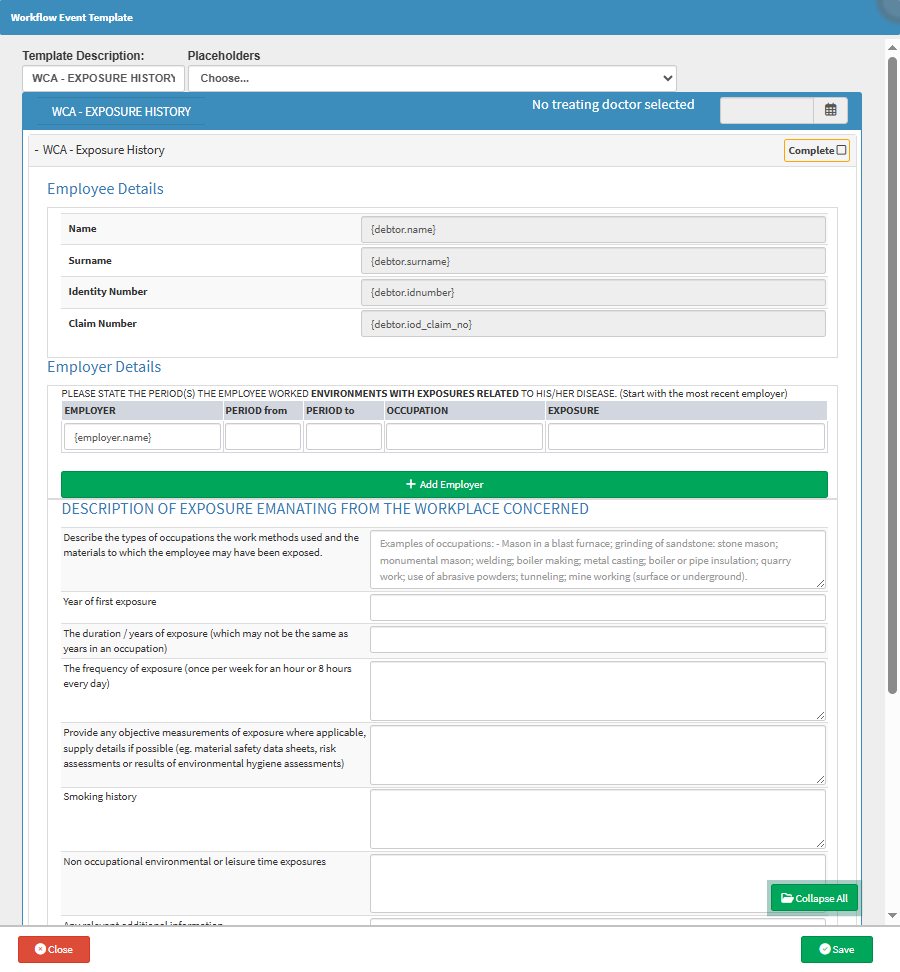
The WCA - Exposure History template ensures that all relevant environmental and occupational factors contributing to the Patient’s disease are thoroughly and accurately captured. It allows the Practitioner to tailor the form to specific industries, hazards, or timelines, ensuring no critical exposure details are missed. This not only strengthens the validity of the compensation claim but also aids in identifying patterns or risks in the workplace, helping prevent future cases.
The WCA - Final template allows you to tailor the form to suit different case complexities and reporting standards. It ensures that all critical information, such as long-term impact, treatment outcomes, final diagnoses, and return-to-work readiness, is captured accurately and efficiently. It also streamlines compliance with Workman’s Compensation Fund requirements and reduces administrative headaches.

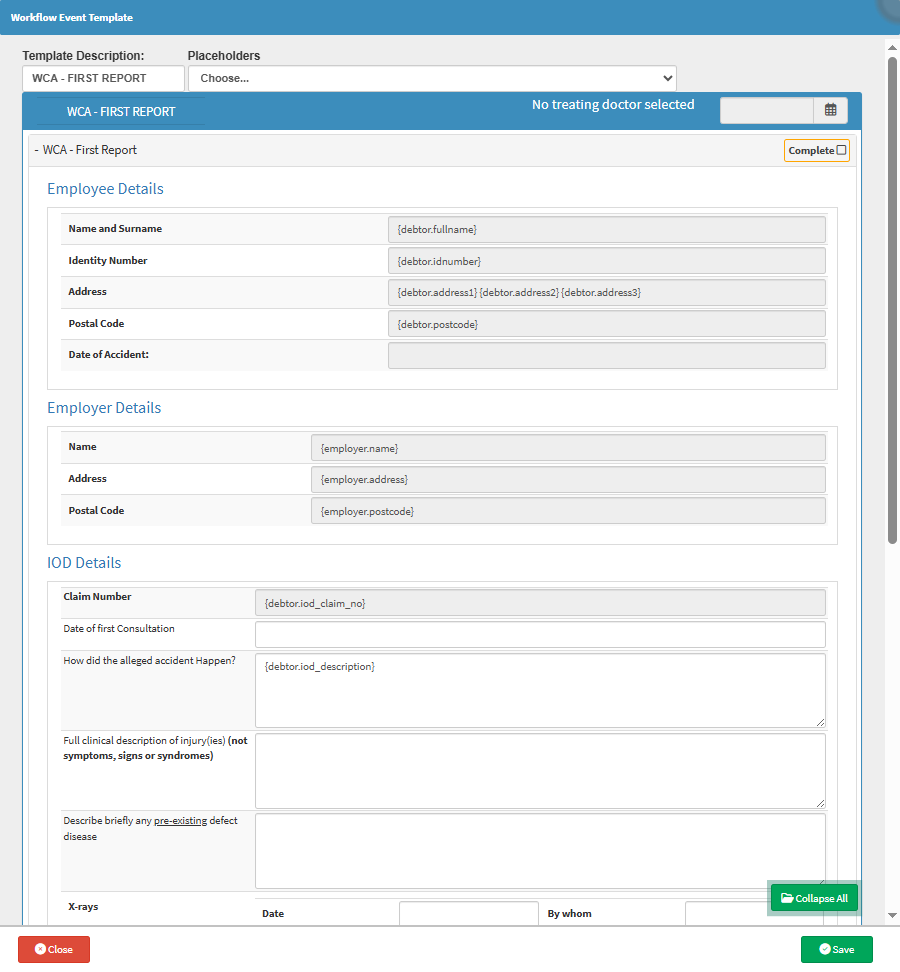
The WCA - First Report template ensures that every relevant detail is accurately recorded while allowing flexibility to adapt to different injury scenarios or practice workflows. It reduces the risk of missing mandatory information, streamlines submission to the Workman’s Compensation Fund, and helps Practitioners avoid repetitive data entry.
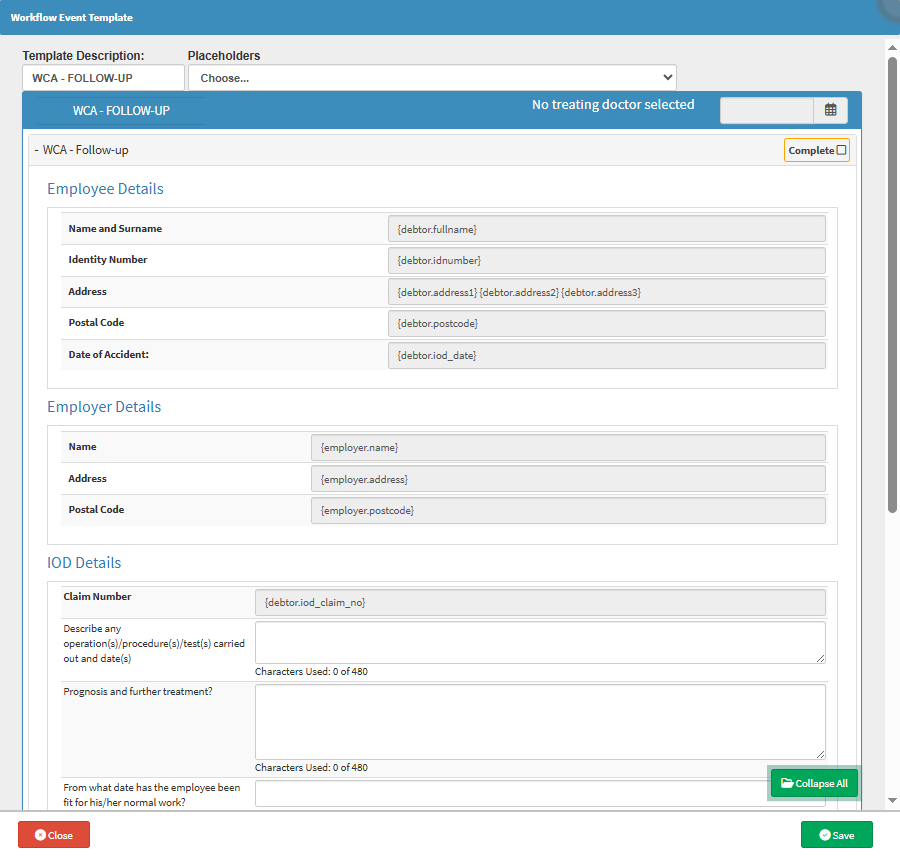
The WCA - Follow-Up template allows you to document changes in the Patient’s condition with precision and flexibility, ensuring that all follow-up actions and findings are recorded. It adapts to varying case complexities, reduces duplicated effort, and ensures compliance with reporting standards.