Best Practice Guidelines: Healthcare Practice Management & POPIA Compliance Framework
Best Practice Guidelines: Healthcare Practice Management
&
POPIA Compliance Framework
Copyright © 2021 GoodX Software. All rights reserved.
GoodX online Learning Centre
learning.goodx.co.za
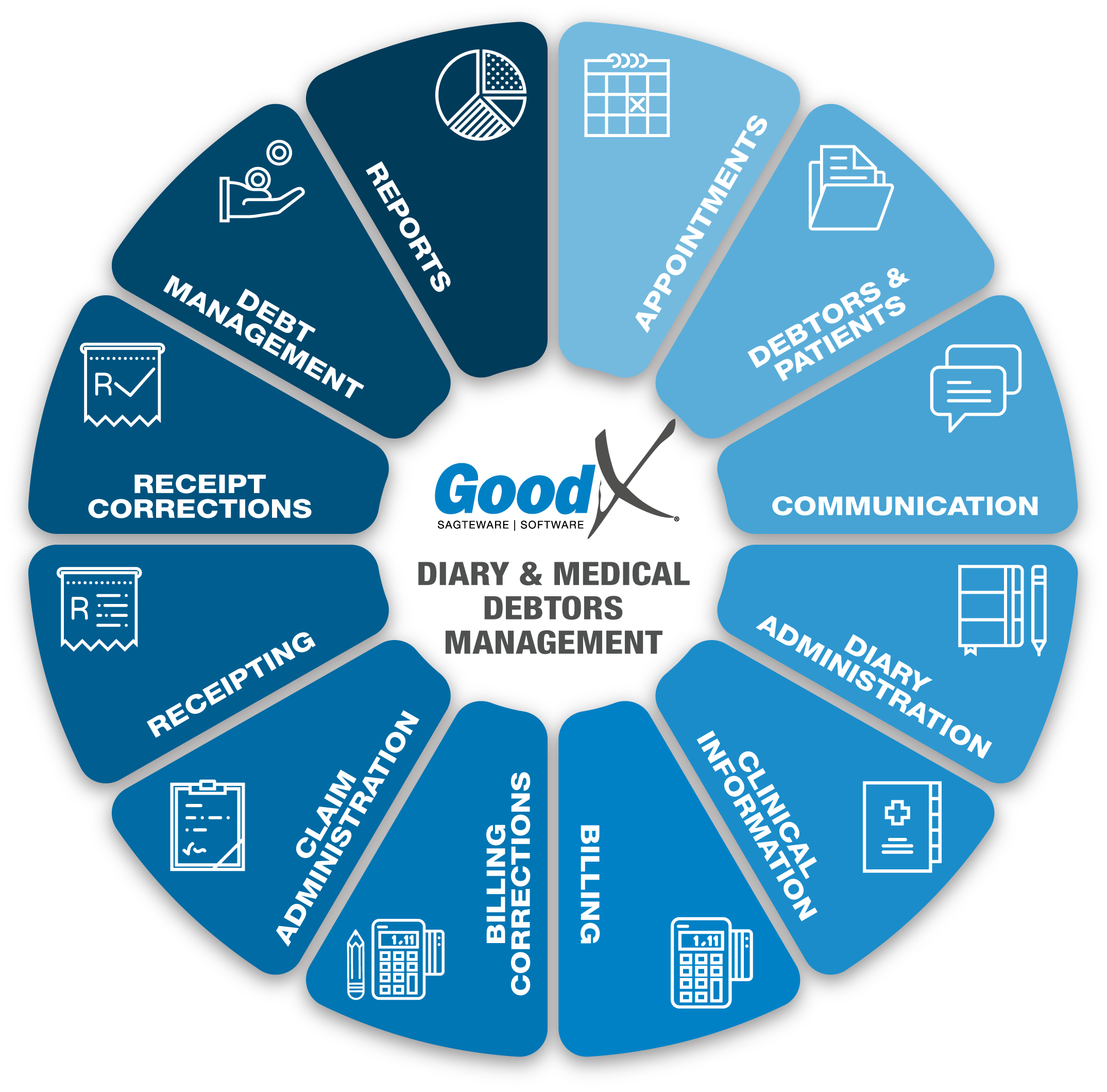
8. Clinical Information: Roles & Purpose
8.8. Clinical History & Reports
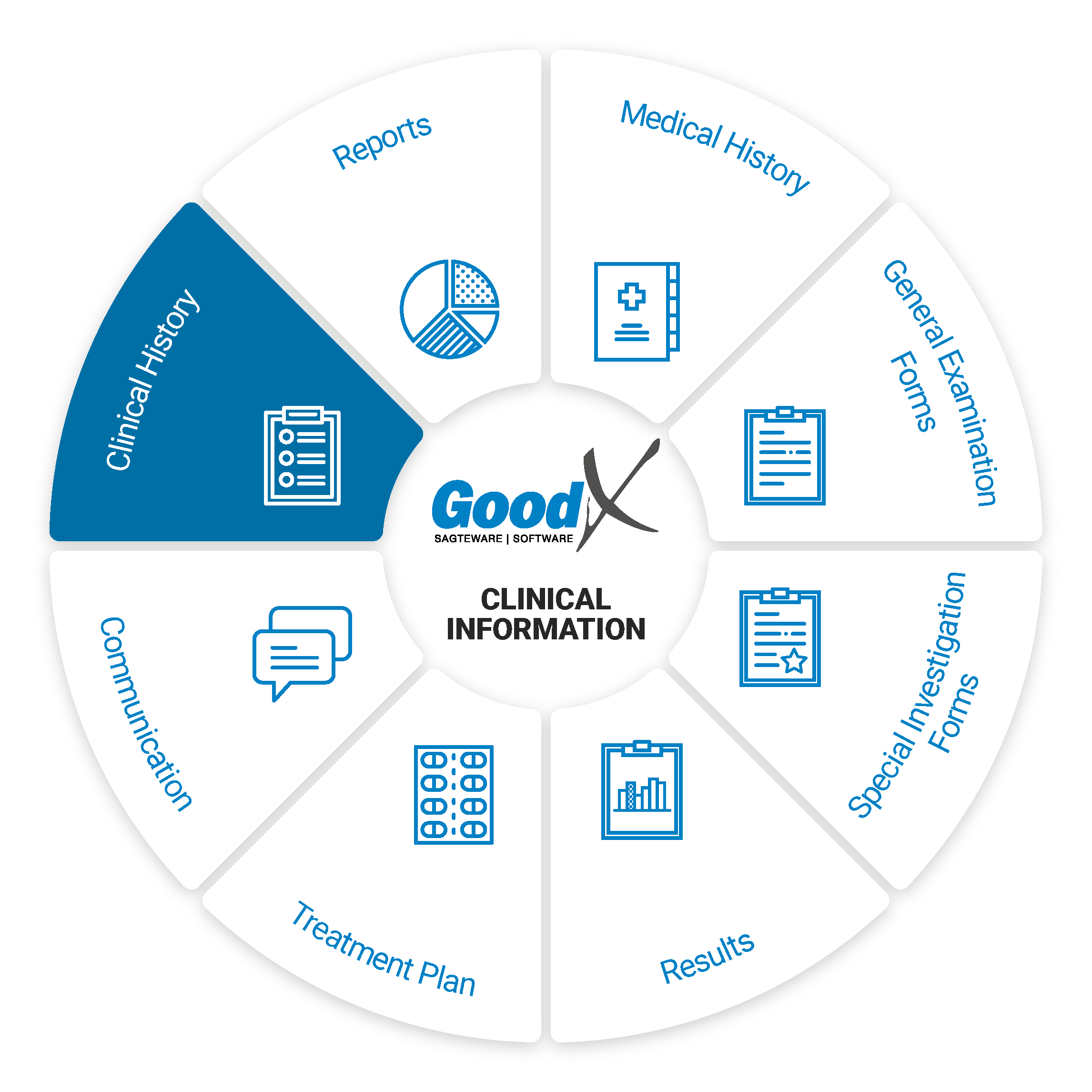
Clinical History
A patient’s clinical history is compiled of all of their past clinical documents.
A patient’s clinical history can assist the practitioner with the treatment of the patient by giving the practitioner a view of the patient’s treatment over a specific time period.
A practitioner is also legally bound to keep a patient’s health records for no less than 6 years and up to 20 years for certain specialities.
Clinical History allows the Practitioner to see all previous medical records of a Patient. Clinical History allows the Practitioner to access and store the Patients' Clinical Events, such as previous scripts, sick notes, investigation forms etc. and when the Patient was at the practice last. The Clinical History can give the Practitioner an indication of what might be wrong with the Patient and can advise the Practitioner what health issues the Patient might be at risk for.
Having a complete Clinical History is critical to keep track of a Patients' general health as it assists the Practitioner in future treatments. The practitioner will also have access to a Patients' Allergies and Chronic Conditions. Adding Clinical History can also assist when a patient is unconscious and not able to communicate what their medical conditions are. This will assist the treating practitioner to determine how to treat the Patient.
Web App
Clinical History
The patient’s clinical history is displayed as a timeline of clinical events (i.e. scripts, sick notes, general examinations, pathology, etc). All clinical history events can be emailed, printed and viewed. Some events can be edited and others like scripts can be copied to a new event of the same type. Some events (e.g. general examinations and pathology) contribute plottable data to the patient’s clinical history and that data can then be viewed from the clinical history in graph/table format so that similar data for a specific period can be easily compared.
Patient Dashboard
The Patient Dashboard is a screen that will display when the user wants to quickly access a Patient's records. Patient Dashboard is a great tool for creating a single location for displaying important medical data you view on a regular basis.
Desktop App
Under the history tab, the patient’s clinical history/notes will be displayed. The procedures, materials and medications that were done/used on a patient along with any clinical notes will be stored in this section.
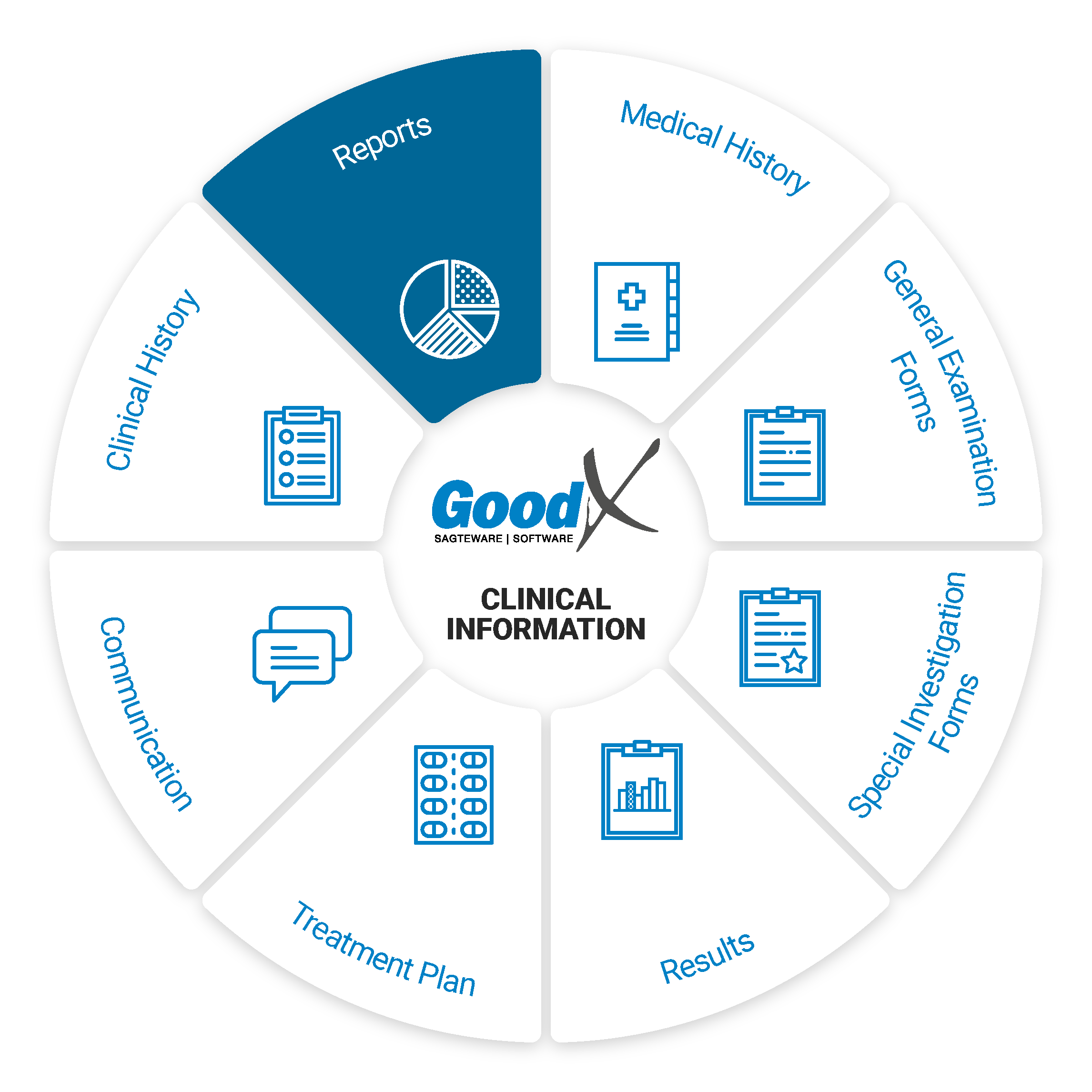 Clinical Reports
Clinical Reports
Clinical reports can be used for letters, such as referral letters, motivation letters, sick notes and much more.
Templates can be used to create any type of letter or clinical report.
The Clinical Report - Pathology Interface is used to access and view the pathology reports from one screen. The user can also manage the results straight from this screen by sending SMS's and emails, calling the patient, or editing/viewing tasks and the pathology report.
Only Desktop App: MS Word is used to create mail merge documents. It is important to note that if you do not have access to MS Word, GoodX can assist you so that your mail merge function can work with LibreOffice.
The history of a patient is collected and stored so that the practitioner can view it in order to have an overview of the patient's medical status.
Autotext Clinical reports: Autotext is used as pre-setup phrases that can be used in the Clinical Reports to quickly type certain information.